

In recent years there has been growing interest in reducing differences in health-related outcomes by race, gender, socioeconomic status, residential location, or other grouping through research, education, and collaboration. Upholding that vision in the course of developing, implementing, and sustaining national health policies is a priority of the current federal administration. Consideration of broad-based legislation that proposes to improve public health and ensure health equity is ongoing. Access to health care resources through universal health insurance coverage and related health promotion provisions are among the most controversial aspects of that legislation.
This article addresses those issues in the context of rural America, specifically as they relate to health outcomes for children in low income families. I argue that access to health care resources, vis-à-vis health insurance, and health promotion issues for children are complex. However, that complexity needs to be given critical consideration if effective health disparity reducing policies are to be adopted and health outcomes improved for rural children.
Health care access issues in rural settings have consistently been characterized by regional concentrations and a combination of factors related to economic well-being. For instance, in a recent study published by the South Carolina Rural Health Research Center (Probst, et al. 2002) it was reported that the prevalence of community-wide economic constraints in high poverty rural areas makes it not only difficult for residents to afford health care services, but also for communities to attract providers. Similarly, in a recent study published by USDA’s Economic Research Service (Jones, et al. 2009), it was reported that rural populations experience lower access to health care along the dimensions of affordability, proximity, and quality, compared to their urban counterparts. Further, lower socioeconomic status contributes negatively to the health status of rural residents.
Those studies and a variety of others produced in the last decade suggest that rural residents face a unique combination of health care disparities not found in urban settings, and thus, policy prescriptions must take that uniqueness into consideration. However, they also add to a wider body of research that in sum provides irrefutable evidence that poverty is related to poor health and that health status improves with increased economic status. While the gradient of change varies, this association has been shown to hold across demographic groups as well as residential locations and different measures of economic status. This implies that while a host of community and individual characteristics may be relevant to accessing health care resources and achieving desirable health outcomes, economic well-being is the dominant factor. It also thereby suggests that health care reform proposals that help to diminish economic inequities may be the most efficacious.
Understanding the potential for any health policy to produce meaningful change, however, is complicated by the fact that there are several pathways through which health outcomes may be affected. For example, extending health insurance coverage to all may reduce the number who are denied medical services or forego necessary treatment altogether due to affordability issues. It may also influence the decision process of individuals with regard to health promoting behaviors. For instance, having health insurance may increase the likelihood that a poor individual will seek preventative care, such as through regular medical check-ups. In either case the impact of economic inequities at the individual level on health outcomes and associated disparities due to insurance coverage may be minimized.
That premise that health insurance coverage is an important predictor of health behavior and resultant health outcomes is regularly used to argue in favor of related policy proposals. Yet, a growing body of research suggests that the aforementioned relationship between economic status and health status remains unchanged after controlling for health insurance. The evidence is particularly strong with respect to children (Bauman, Silver, and Stein 2006). This raises several pertinent policy research questions, such as: What is the direct impact of health insurance coverage on health status? What is the net effect of health insurance on health status given its potential to influence health promoting behaviors? What is unique about children that make it less likely that change in health outcome disparities will result from increased health insurance coverage?
The last question can be answered in part by the fact that child health has unique characteristics that differentiate it from adult health, and therefore, health care issues for children are not identical to those for adults (U.S. Department of Health and Human Services 2004). For instance, there are many stages of development and growth through which children pass in a relatively short period of time. Healthy completion of each stage of that process is an important determinant of health in the next. Therefore, the timing of increased access to health care through insurance may be more critical to children’s health than to that of adults. Further, children’s basic physiology differs from that of adults, as demonstrated by age specific patterns of health, illness, and disability, all of which create differential quality-of-care problems.
Another characteristic is that children’s health care is dependent on adults. They depend on the decisions and actions of adults with respect to accessing health care and the consistency of that care in terms of timeliness, follow-through, coordinating care, and ensuring preventive services. Continuity of care is also an issue for children. Unlike adults, children tend to receive health care in a multitude of environments, such as in health clinics, in school, and in the home, where health insurance coverage may be less relevant to receipt and quality of care. Additionally, the development of good or bad health behaviors in children is dependent on exposures, such as diet, exercise, smoke, violence, and other factors that are associated with and impacted by family behaviors.
Lastly, poverty alone increases the complexity of health issues for children and may thereby increase the likelihood that health status disparities will persist despite policy intervention. Children make up more than one-third of the nation’s poor and child poverty rates are consistently higher in rural than in urban areas. The full impact of that poverty on the well-being of rural children during adolescence and over their life course is not known, but there is ample research to suggest that their overall health is significantly compromised in comparison to children of nonpoor families. For example, poor children have been shown to have higher rates of obesity, chronic disease, and mortality and lower rates of comprehensive and consistent health care coverage than their nonpoor counterparts. They have also been shown to have lower levels of engagement with health promoting behaviors, such as exercise and preventative medical exams.
Far less is known about those differences given the depth and extent of family poverty. A broad range of consequences of low income have been documented in prior health disparities research, but that research has tended to focus on poor versus nonpoor groups. Yet, low-income populations are not easily divided along those lines when considering federal policy. Differences exist with respect to source and level of income, recipient age, and family structure when it comes to eligibility for participation in social assistance programs. Thus, without going into statistical detail, it is fair to conclude that the health related benefits of those programs, such as food stamps and public health insurance, are not equally available to and accessed by all poor families with children. Further, some of those benefits are accrued by nonpoor, low-income families.
The impact of program eligibility on health outcomes may influence the ability for increased health insurance coverage to reduce disparities. In other words, the maximum return on health insurance coverage alone may have already been reached for some children among the poverty population through existing federal policy, but not for others. Recognizing that along with the combination of unique characteristics of rural, child, and poverty populations, is critical in the evaluation of proposed health reform policy. Data from the 2007 National Survey of Children’s Health are used here to illustrate the benefits of taking the complexity of those relationships into consideration (U.S. Department of Health and Human Services 2009). The details of this analysis are discussed in brief in order to focus the remainder of the article on summarizing the key findings and their implications.
Selection of cases to be analyzed is based on rural residence and family income below 200% of the federal poverty level. Three income groups are produced from the sample: low-income, nonpoor families; working poor families; and nonworking poor families. For each group, descriptive statistics, graphical path analysis, partial least squares regression, and statistical decomposition are used to answer the two remaining research questions: What is the direct impact of health insurance coverage on health status? What is the net effect of health insurance on health status given its potential to influence health promoting behaviors?
The indicators for health insurance coverage include the existence of any health insurance coverage, the adequacy, consistency, and type of health insurance coverage if any, and associated out of pocket expenses. Child health promoting behaviors include preventative medical and dental examinations, sleep patterns, and exercise habits. Health promoting behaviors in the family environment include parental health status, exercise habits, and the smoking habits of all family members. Health status consists of perceived health of the child, activity limitations, presence of chronic disease/illness, and body mass given height/weight by age. Several demographic characteristics are also used in the analysis: child’s age and race, parental education and nativity, and family structure.
The descriptive statistics show that the likelihood of having any health insurance coverage at all is not significantly different among the three income groups. However, differences exist with respect to type and adequacy of insurance coverage as well as out of pocket costs. All of the child health indicators and demographic characteristics are found to be significantly different among the income groups, as are all health promoting behaviors except for child sleep. These findings suggest that factors other than just having health insurance coverage are relevant to rural child health status, but where health insurance coverage exists, aspects of that coverage may be influential in determining both behaviors and outcomes. These conclusions are confirmed by supporting analyses.
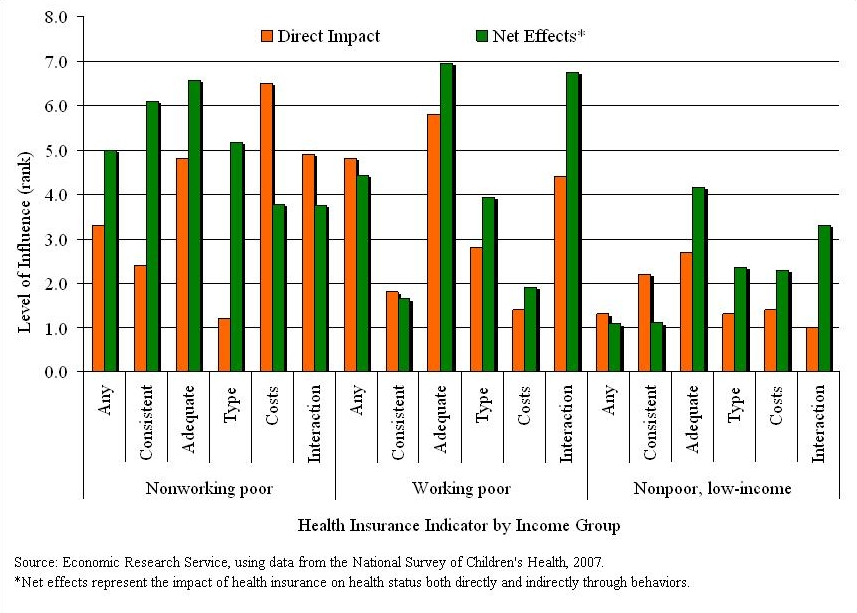
A statistical summary of those analyses is presented in Figure 1. The values on the vertical axis represent a scale of 0 to 10, where 10 is the most influential aspect of insurance coverage on child health status overall and 0 the least influential. Given that, out of pocket costs have the greatest direct impact (6.5) on child health for nonworking poor families. Yet, it is the least influential when considering net effects (3.8). Adequacy is second for direct impacts (4.8), but it is the most influential for net effects (6.6).
The difference between the direct and net values is explained by the influence of health insurance adequacy on health promoting behaviors and the manner in which those behaviors influence health status. In other words, if the influence of adequacy of insurance on behavior was not considered then its relevance to overall health status for children of nonworking poor families would be underestimated by 27%. Comparatively, the influence of out of pocket costs would be overestimated by nearly 42%. However, the difference between the two measures is greatest for type of insurance, with an estimated direct impact of 1.2 and 5.2 for net effects. Therefore, failing to consider the impact of type of health insurance—public or private—on health status through health promoting behaviors would render it nearly 77% less influential. Similarly, consistency of insurance and having any insurance coverage at all would be underestimated by nearly 61% and 34%, respectively.
Adequacy is also the most influential for children of working poor families. This is found to be the case for both direct impacts (5.8) and net effects (6.9). The same is found to be true for children of nonpoor, low-income families, but to a lesser degree (2.7 direct and 4.2 net). Overall, each of the insurance indicators is found to have some independent measure of effect on rural children’s health status, either directly or indirectly through health promoting behaviors, for the three income groups. However, when considering the interaction of all of the health insurance coverage indicators used in the analysis, their combined influence is found to be greatest for children of working poor families (6.7 net). This suggests that on the whole, quality of insurance matters especially for children of working poor families.
These findings lend support to the premise that health insurance coverage is an important predictor of health behavior and resultant health outcomes. In so doing, they also suggest that conjoined policies that seek to increase the rate of insurance coverage and health promoting behaviors will have a greater impact on the health outcomes of children in low-income rural families than increasing insurance coverage alone. Further, the magnitude of that impact will likely be greatest for children of working poor families, which in turn may help to reduce health outcome disparities between poor and nonpoor income groups as well as within low-income groups.
With respect to the relevance of health insurance coverage in general, it can be concluded that health insurance availability is less important than the quality of the insurance in determining health outcomes. This conclusion points to the importance of policy discussions that consider type, consistency, and adequacy of insurance, as well as other related factors. Likewise, research used to inform health policy must go further to provide an understanding of the degree to which those factors serve as mediators of health promoting behaviors and thereby indirectly influence health outcomes. Lastly, if health disparities are to be addressed then information about the manner in which certain policies are most appropriate and their potential effect on sub-populations is essential.
In that regard, the study touched upon in this article argues for research-based social policy; whereby a behavioral approach is in some way integrated and carried out in developing health care policy. In this instance, for example, the likelihood that health insurance will influence health promoting behavior is greatest for nonworking poor families given the consistency of insurance coverage. However, considering the estimated net effects in relation to health outcomes, adequacy of insurance is found to be most influential across all low-income groups. This suggests that an effective and efficient health promotion policy aimed at serving children in rural low-income families would be that which targets improvements in both the comprehensiveness and quality of health care coverage. Further, if reducing health inequities within the rural low-income population is a policy goal, then inconsistency of health insurance coverage must also be addressed.
Bauman L.J., E.J. Silver, and R.E.K. Stein. 2006. Cumulative social disadvantage and child health. Pediatrics 117(4), pp. 1321-8.
Jones, C., Parker, T., Ahearn, M., Mishra, A., and Variyam, J. (2009) Health status and healthcare access of farm and rural populations, EIB-57. Washington, D.C.: U.S. Department of Agriculture, Economic Research Service.
Probst, J.C., Samuels, M., Jespersen, K., Willert, K., Swann, R., and McDuffie, J. (2002). Minorities in rural America: An overview of population characteristics. Columbia, So. Car.: South Carolina Rural Health Research Center, University of South Carolina.
U.S. Department of Health and Human Services. (2004). Child health care quality toolbox: why child health measures? Rockville, Md: Agency for Healthcare Research and Quality. Available online: http://www.ahrq.gov/chtoolbx/why.htm
U.S. Department of Health and Human Services. (2009). Design and operation of the National Survey of Children’s Health, 2007. Hyattsville, Md: Centers for Disease Control and Prevention, National Center for Health Statistics.
| Any insurance | Does the child have any kind of health care coverage, including health insurance, prepaid plans, or government plans? |
| Consistent insurance | During the past 12 months was the child consistently insured (any form of insurance), consistently uninsured, or uninsured periodically? |
| Adequate insurance | Are the child's health care needs adequately met/covered by his/her health insurance? |
| Type of insurance | Is the child primarily covered by private insurance, public insurance, or uninsured? |
| Out of pocket costs | Are there current out of pocket costs associated with health insurance and if yes, are they reasonable? |
Source: Economic Research Service, using documentation from the National Survey of Children’s Health, 2007.
The views expressed here are those of the author, and may not be attributed to the Economic Research Service or the U.S. Department of Agriculture.