The success and viability of farm businesses depend to a certain extent on the quality and quantity of the labor force. Promoting a healthy workforce is a priority for U.S. agriculture because hired labor is an essential production input, accounting for the third largest production expense (Kandel, 2008). Recruiting and retaining farm workers, however, has usually presented a difficult challenge for farm businesses given high physical demands, heavy workloads, and relatively lower wages in the agricultural sector (Luo and Escalante, 2017a). These employment challenges are further aggravated by health risks: farm employees work under volatile weather conditions and risk contamination from chemicals in the production and processing environments (Grzywacz, Quandt, and Arcury, 2008).
Maintaining a healthy farm labor force is further complicated by the reality that a majority of workers on U.S. farms are immigrants, some of whom may not even have legal authorization to work or be in the United States (Kandel, 2008; Martin and Jackson-Smith, 2013). Martin (2016), for instance, claims that between 2007 and 2009 only 30% of U.S. crop workers were born in the United States, while the remaining 70% were foreign-born. Within this category, about 55% were unlawfully residing in the United States and did not have legal employment authorization. Notably, jobs in the agricultural sector are 3.5% more likely to be performed by an undocumented worker than by a local, documented worker (Bump, 2015).
Recent stricter implementation of immigrant control policies has resulted in the deportation of some undocumented immigrants (Escalante, Yu, and Li, 2016). At the same time, employment verification systems and monitored hiring procedures have been established and enforced, as have harsher sanctions (involving higher civil fines and criminal penalties) for employers who violate the law (Smith and Sugimori, 2015). However, even with the intensified immigration control enforcement efforts, the share of undocumented workers dropped in only a few industries, such as construction (Passel, 2015).
Given the legal/illegal status profile of the farm sector labor force, understanding the patterns of workers’ health care decisions could illuminate critical health care needs for farm workers. Nurturing a productive farm labor force requires immigrant farm workers’ health care needs and access to be given attention and consideration to a similar extent afforded farm workers who are U.S. citizens (Mohanty, 2006; Mohanty et al., 2005; Laroche, 2000). What health care decisions do farm workers make? Do these decisions vary by legal status? Having this information can provide accurate and specific suggestions for farm operators in their efforts to maintain acceptable health standards among their workers.
As the country’s new leaders contemplate introducing significant changes to the previous administration’s health care policies, the social imperative requires policy-makers to optimally allocate medical resources and promote the health welfare of all agricultural workers. To answer these questions, we first compare the health care utilization patterns of green card and undocumented farm workers with those of citizen farm workers who may be less constrained in accessing health services and benefits. The increasing immigrant population in the United States has created strong public sentiment due to the adverse effect on the adequacy and cost of social welfare programs (Borjas 1999). Given the implementation of public health reforms (e.g., the Personal Responsibility and Work Opportunity Reconciliation Act of 1996) and stringent immigration enforcement (e.g., E-verify mandates), do immigrants enjoy access to health care services and rates comparable to those enjoyed by U.S. citizens? We answer this question by investigating farm workers’ choices among health care provider alternatives and the payment methods they use to settle health care bills. Based on legal status and demographic characteristics, farm workers may have diverse preferences for health care providers and methods of payment.
The availability of adequate and reliable health insurance coverage enhances a farm worker’s access to health care services and provides relief in the settlement of health care bills. In addition to existing public health programs—such as Medicaid, Medicare, and military health care plans—a farm worker’s options may also include employer-provided health insurance (EPHI) or directly purchased health insurance (DPHI).
EPHI is a major means of providing employee health insurance coverage in the United States and covers over 54% of the U.S. population (Smith and Medalia, 2014). Among working-age adults (ages 18–64), the overall EPHI coverage rate for U.S. citizens is 67%, compared to 46% among legal permanent residents and 31% among undocumented immigrants (Capps, Rosenblum, and Fix, 2009). Immigrant workers are less likely to be covered by EPHI because 40% of them work in construction or agricultural industries, which generally have lower EPHI coverage rates (Ku and Jewers, 2013). The Affordable Care Act (ACA) passed in 2010 mandated that employers with at least 50 employees must provide health insurance coverage to full-time employees and their dependents. But the ACA excluded companies in the farm and service industries that either hired fewer than 50 employees or depended on seasonal workers. The 2012 annual average number of hired workers per farm business ranged from 18.5 to 85.8 in the sixteen farm labor regions (excluding state-level estimates provided separately for California and Hawaii) defined under the NASS farm labor survey system. Only three regions (Pacific, Lake, and Southern Plain) reported an average of more than 50 workers per firm (USDA-NASS, 2012).
Directly purchased health insurance (DPHI) is a costly but important alternative for individuals in the United States who not eligible for both EPHI and public health insurance programs. According to Smith and Medalia (2014), 11% of the U.S. population choose DPHI and paid the premium out-of-pocket in 2010.
U.S immigrant health care policies are inextricably linked to the effectiveness of the public health insurance program, which the Trump administration has explicitly targeted for a significant overhaul. A major immigration policy reform in 1996, the PRWORA1996, requires a five-year waiting period for all lawful permanent residents to be eligible for Medicaid and Children’s Health Insurance program (CHIP), regardless of financial situation. Undocumented immigrants remain ineligible for all public insurance programs (Ku, 2006). As a result, immigrant workers, especially those who are undocumented, have lower rates of health insurance coverage than citizens (Derose, Escarce, and Lurie, 2007).
Source: National Agricultural Workers Survey, 2007-2012
Source: National Agricultural Workers Survey, 2007-2012
The demographic and health-related profiles of about 28,000 farm workers were compiled from National Agricultural Workers Survey (NAWS) annual datasets from 2007 to 2012. Workers fall into three legal status classes: citizens, green card holders, and undocumented workers.
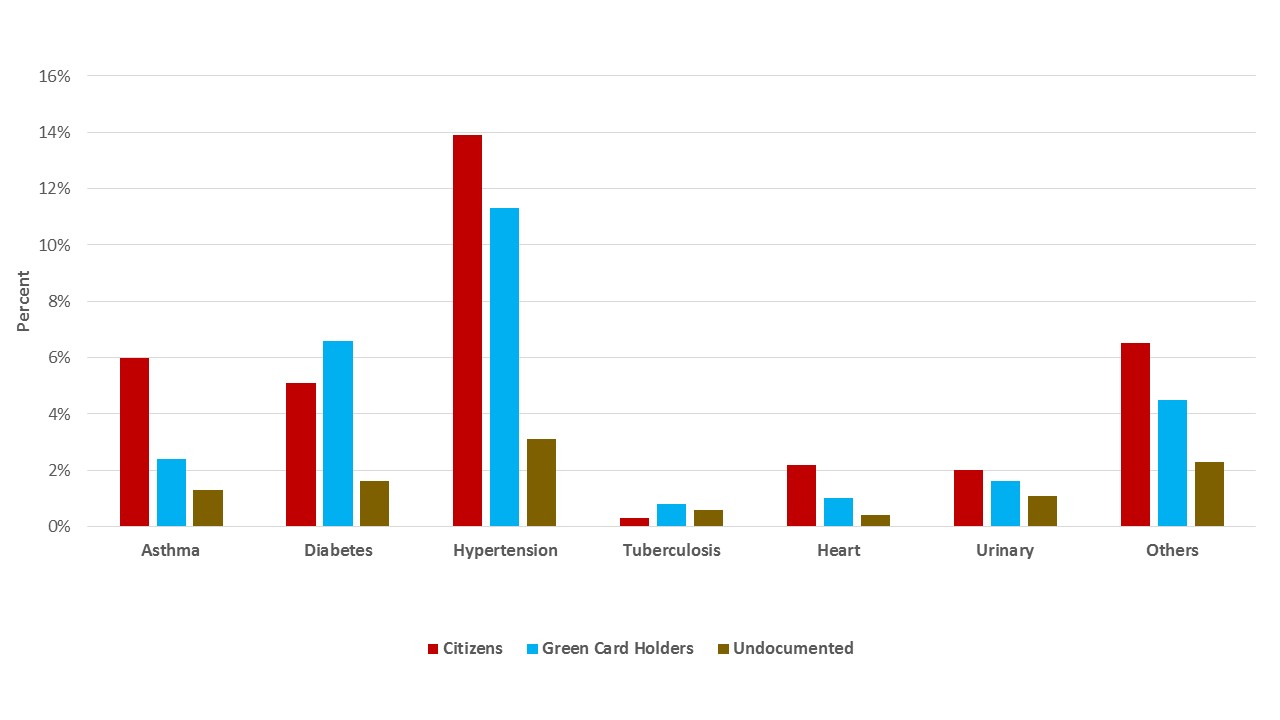
Based on average demographic attributes, undocumented workers are usually younger, with an average age of 30 years, relative to other workers, who are at least 10 years older on average. The age profile of undocumented workers is supported by the supposition that younger people are healthier and thus more likely to migrate to where there is work (McDonald and Kennedy, 2004). This would also explain the small incidence of chronic diseases (e.g., asthma, diabetes, and hypertension) among the younger undocumented cohorts compared to the other groups of workers as compiled from the NAWS (Figure 1). Better health status of undocumented farm workers may result in lower utilization rate of health care services than that of the average U.S. citizen of the same age.
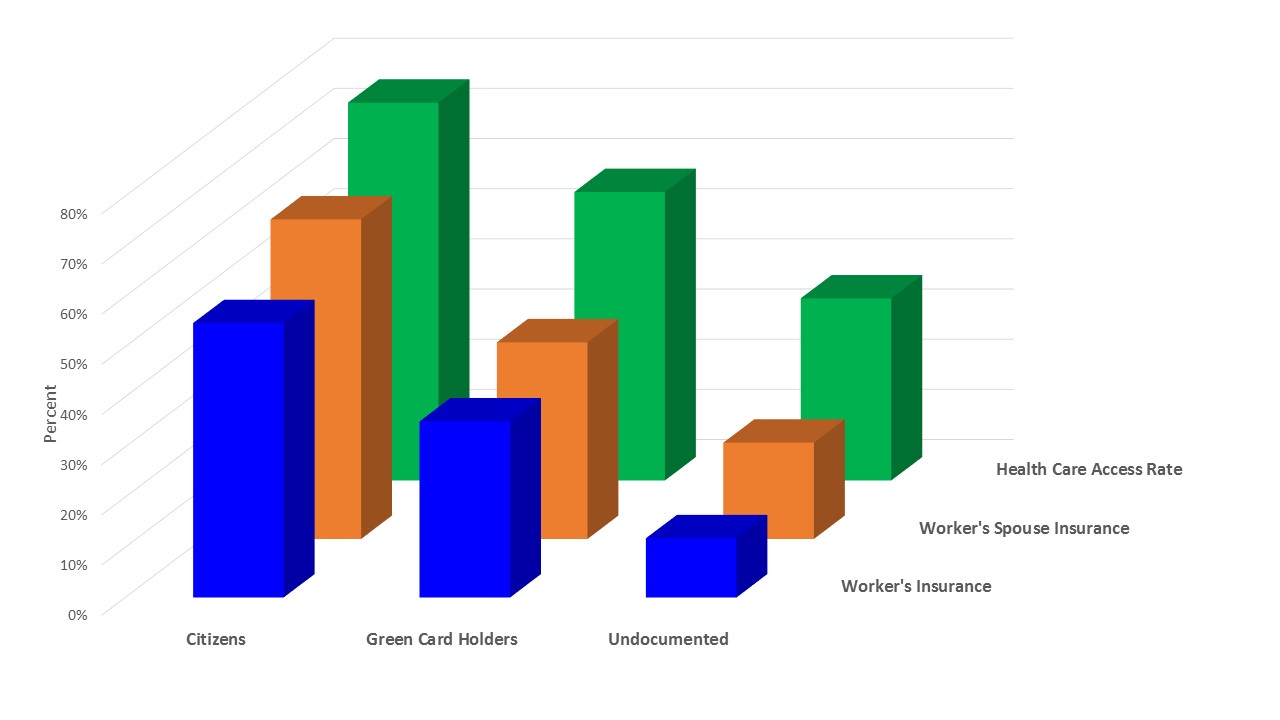
The NAWS dataset also provides information on health insurance coverage for farm workers and their spouses. The indicator of health insurance availability considers a farm worker’s acquisition of single or multiple coverage of public (e.g., Medicaid and Medicare) and private (e.g., EPHI and DPHI) health insurance. In the United States, EPHI coverage can also be extended to spouses and children, which creates a reliable health insurance bond between farm workers and their families. Moreover, in regard to public health insurance such as Medicaid, if one person in the household is eligible, there is a higher chance that the spouse may also be able to benefit from a public health insurance plan. Even if only one person is eligible, it would increase the chance that additional coverage would be purchased to cover other family members. The trends in Figure 2 confirm a large discrepancy in health insurance availability among the different legal classes of workers. Citizens usually enjoy more access to health insurance coverage opportunities, while undocumented workers experience more hurdles and constraints in obtaining health insurance, whether these were obtained by the workers themselves or through their spouses.
The health care utilization rate for undocumented workers is significantly lower compared to that of other workers. This is validated by the trends in the workers’ rate of access to health care services during the two-year period prior to the start of the 2007 survey. Figure 2 shows that citizens registered the highest frequency rate of health care use (75.3%), while undocumented workers had the lowest frequency rate (36.3%).
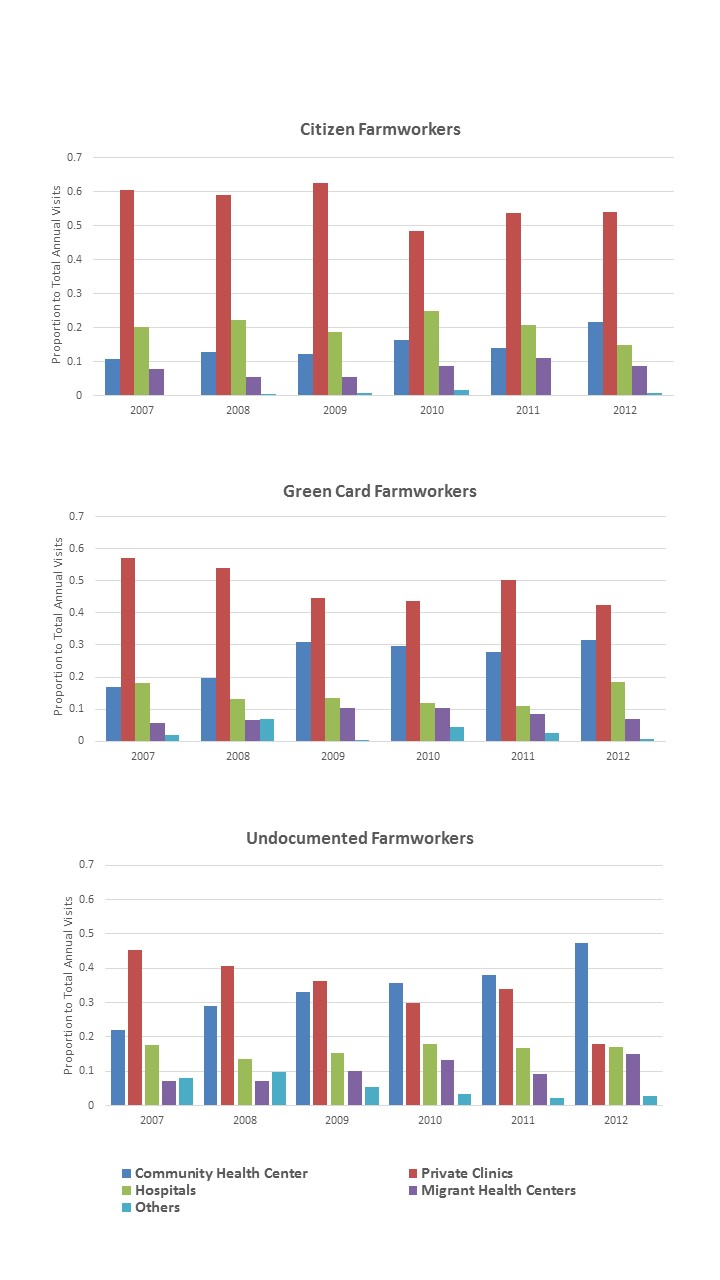
If certain farm workers experience more constrained access to health care services than others, which service providers do they rely more on for their urgent health concerns? Figure 3 presents separate plots of the annual health care provider choices among citizen, green card, and undocumented farm workers (calculated as the proportion of visits made to each service provider alternative to total visits) from 2007 to 2012.
Citizen and green card workers had almost identical patterns of health provider selection, notably the consistently higher patronage of private hospitals, during the six-year period. The only deviation in these workers’ choices can be observed during the last four years of the time period, when green card holders started increasing their patronage of community health centers. Such modified choices could have been induced by tighter household budgets and income constraints due to the effects of the recession and its aftermath.
With their lower socioeconomic status and constrained mobility, undocumented workers find themselves in a more disadvantageous position in accessing social resources, especially during recessionary periods (Massey, Gross, and Shibuya, 1994). Figure 3 indicates that these workers are initially inclined to use the relatively more costly private clinic services for most health care needs. Interestingly, this choice could have been influenced by their need for less visibility to immigration enforcement authorities, as legal identities are not essential requirements for receiving services at these clinics. During the recession (from 2009 onwards), however, these workers have relied more on community health centers, which were apparently the more affordable option during those times. These workers also used migrant health centers at higher rates than the other two worker groups, but these rates did not exceed their utilization rates for private clinics and community health centers. These trends can be partly attributed either to the inadequacy of extensive or comprehensive medical services at these centers or the need to elude immigration authorities, who may have closely monitored activities because of the possible presence of deportable undocumented persons in such places.
Source: National Agricultural Workers Survey, 2007-2012
Source: National Agricultural Workers Survey, 2007-2012
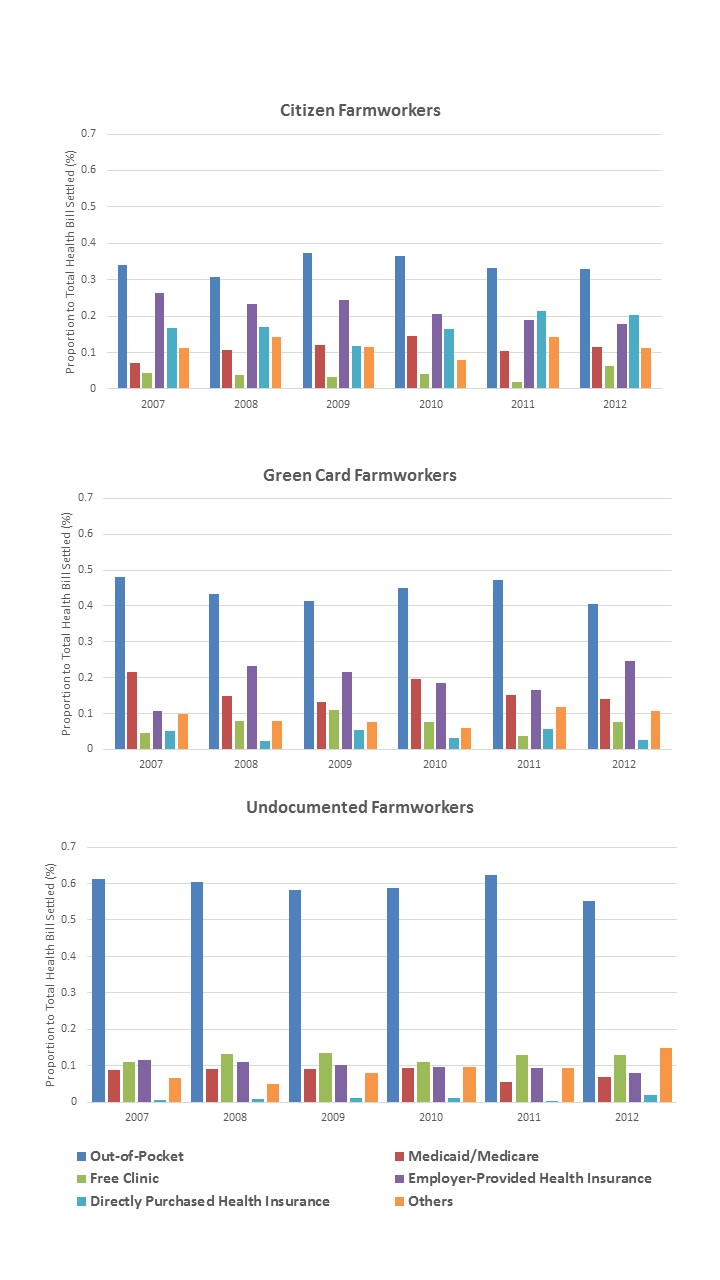
Given workers’ varied preferences for certain health service providers, their usual payment arrangements for settling their health care services bills can also provide important indications of motivations and choices, thus leading to financial and welfare implications. As can be seen in Figure 4, farm workers in general have a high probability of paying for health care services using their own funds, with undocumented farm workers registering the highest probability at 48%. For those with legal immigration status, this could be caused primarily by lack of health insurance. Workplace hazards and risks raise health insurance premiums significantly, such that farm workers could have been discouraged from purchasing any individual health plan (Sundaram-Stukel and Deller, 2009). Only 32.6% of farm workers actually enjoyed EPHI benefits in 2010. This rate is considered low compared to management and professional jobs, where 89.4% of workers are provided health services benefits (U.S. Census Bureau, 2010). Without any health insurance plans, even farm workers with legal immigration status may need to absorb all medical costs themselves.
In Figure 3, EPHI is the second most frequently used payment method by citizens and green card holders in most years, although this option’s probability is less than half of that of out-of-pocket payments. Green card holders also use more Medicaid/Medicare assistance than the other two worker groups. Given their lower average reported incomes in the NAWS datasets compared to citizens, they may have resorted to avail themselves of such payment relief services after they have completed the five-year residence requirement for availing of certain public health benefits.
Undocumented workers are least accommodated by EPHI benefits at the discretion of some employers because U.S. labor laws only guarantee these workers basic rights, which exclude such benefits (Contreras, 2015; Bray, 2016). Their conditions are compounded by their illegal immigration status, which inhibits them from accessing any public benefit programs such as Medicare. As a result, undocumented workers are most likely to pay for health care costs out-of-pocket. As Figure 4 indicates, their personal funds account for a much larger proportion of their health bill payments compared to other workers. The average proportion of this payment option for these workers is almost 60%, while citizens and green card holders pay average out-of-pocket rates of only 34% and 44%, respectively.
The goal of sustaining a healthy farm workforce is an important policy consideration given the sector’s dependence on labor inputs. This priority is a challenge that must consider several issues. First, replacing foreign workers could be complicated due to difficulties in sourcing and hiring domestic workers to replace displaced undocumented workers. Citizens and green card holders have usually been unwilling to endure demanding, strenuous farm work in favor of better pay, more employee benefits, and more favorable working conditions in other industries (Wozniacka 2013; Wells 2012). When documented domestic workers are hired, some farmers have had to contend with levels of farm labor productivity that are significantly lower than those achieved by former undocumented workers. In less mechanized operations, large quantities of crops remained un-harvested and resulted in huge crop losses (Preston, 2007; McKissick and Kane, 2011).
Second, employing foreign labor (except those sourced under the H2A guest farm worker visa program) translates to substantial farm cost savings. Wages for documented workers in fruit, nut, and vegetable farms are 18% higher than wages for undocumented workers (Ruark and Moinuddin, 2011).
Third, retaining farm workers is a pressing concern in the farm sector, especially in the more labor-intensive fruit, vegetable, and horticulture industries. In their analysis of farm labor turnover trends by analyzing workers’ employment time allocation between farm and non-farm work, Luo and Escalante (2017a) found that citizen and green card farm workers tend to have significantly lower workweek allocations to farm work than undocumented workers. During periods of economic downturn, citizens and green card holders further reduce their workweek allocation to agricultural employment as they explore more financially rewarding job opportunities in the non-agriculture sector. In contrast, undocumented farm workers are usually much less responsive to economic shocks as they tend to stick to their status quo labor allocation pattern (favoring farm employment) during such difficult times.
Finally, even during the Obama administration, legislative policies (such as the PRWORA96) were already being enforced to restrict immigrants’ access to public benefits. These policies were intended to quell growing concern that the increasing presence of immigrants in the country could deprive many domestic residents, especially citizens, of necessary health care and public services (Borjas, 1999). Given the Trump administration’s stronger immigration stance, more restrictive policies could further diminish foreign workers’ access to welfare resources, including health care services.
Such policies, if indeed implemented, could have serious negative repercussions on the agricultural sector, which relies heavily on immigrant workers, especially for seasonal farm work (Martin and Jackson-Smith, 2013). In addition, the reality is that a disconnect exists between the sector’s actual provision of health insurance benefits to its workers and farm workers’ more physically demanding, riskier, and more taxing workloads (Grzywacz, Quandt, and Arcury, 2008; Luo and Escalante, 2017b). Even if foreign workers in the farm sector were replaced entirely by domestic workers, the persistent reality is that these replacement workers and their dependents are not adequately covered with insurance through their EPHI benefits and thus would resort to making health care decisions based on their own financial resources. In the absence of more reliable health insurance, health care, and public service programs, the agricultural sector confronts the issue of maintaining a healthy workforce as its deterioration could have a negative impact on labor productivity, the sector’s viability, and the nation’s domestic food supply.
Anton, J. I., and R. M. Munoz de Bustillo. 2010. “Health Care Utilization and Immigration in Spain.” European Journal of Health Economics 11:487–498.
Borjas, G. 1999. “Immigration and Welfare Magnets.” Journal of Labor Economics 17(4):607–637.
Bray, I. 2016. “Legal Rights of Undocumented Immigrants.” Lawyers.com, New Providence, NJ: Martindale-Hubbell. Available online: http://immigration.lawyers.com/general-immigration/legal-rights-of-illegal-immigrants.html
Bump, P. 2015. “Where America’s Undocumented Immigrants Work.” The Washington Post. Available online: https://www.washingtonpost.com/news/the-fix/wp/2015/03/27/where-americas-undocumented-immigrants-work
Capps, R., M. R. Rosenblum, and M. Fix. 2009. Immigrants and Health Care Reform: What’s Really At Stake? Migration Policy Institute. Available online: http://www.migrationpolicy.org/research/immigrants-and-health-care-reform-whats-really-stake
Contreras, R. L. 2015. “Yes, Illegal Aliens Have Constitutional Rights.” The Hill. Available online: http://thehill.com/blogs/pundits-blog/immigration/255281-yes-illegal-aliens-have-constitutional-rights
Derose, K. P., J. J. Escarce, and N. Lurie. 2007. “Immigrants and Health Care: Sources of Vulnerability.” Health Affairs 26(5):1258–1268.
Escalante, C. L., Y. Wu, and X. Li. 2016. “Organic Farms’ Seasonal Farm Labor Sourcing Strategies in the Pre-“Arizona” Mode of Immigration Control.” Applied Economics Letters 23(5): 341–346.
Grzywacz, J. G., S. A. Quandt, and T. A. Arcury. 2008. “Immigrant Farmworkers' Health-Related Quality of Life: An Application of the Job Demands-Control Model.” Journal of Agricultural Safety and Health 14(1):79–92.
Kandel, W. 2008. Profile of Hired Farmworkers: A 2008 Update. Washington, D.C.: U.S. Department of Agriculture, Economic Research Service, Economic Research Report 60, July.
Ku, L. 2006. Why Immigrants Lack Adequate Access to Health Care and Health Insurance. Migration Policy Institute. Available online: http://www.migrationpolicy.org/article/why-immigrants-lack-adequate-access-health-care-and-health-insurance
Ku, L., and M. Jewers. 2013. Health Care for Immigrant Families: Current Policies and Issues. Washington, D.C.: Migration Policy Institute.
Laroche, M. 2000. “Health Status and Health Services Utilization of Canada’s Immigrant and Non-Immigrant Population.” Canadian Public Policy/Analyse de Politiques 26(1):51–75
LeClere, F. B., L. Jensen, and A. E. Biddlecom. 1994. “Health Care Utilization, Family Context, and Adaptation among Immigrants to the United States.” Journal of Health and Social Behavior 35(4):370–384.
Luo, T., and C. L. Escalante. 2017a. “US Farm Workers: What Drives Their Job Retention and Work Time Allocation Decisions?” Economic and Labour Relations Review, in publication process.
Luo, T., and C. L. Escalante. 2017b. “Employer-Provided Health Benefits and the Employment Decisions of U.S. Farm Workers.” Agricultural Finance Review, in publication process.
Martin, P. 2016. “Immigration and Farm Labor: Challenges and Opportunities.” AgBioForum 18(3), 252-258.
Martin, P., and D. Jackson-Smith. 2013. Immigration and Farm Labor in the U.S. East Lansing, MI: National Agricultural and Policy Development Center, Michigan State University.
Massey, D. S., A. B. Gross, and K. Shibuya. 1994. “Migration, Segregation, and the Geographic Concentration of Poverty.” American Sociological Review 59(3):425–445.
McDonald, J. T., and S. Kennedy. 2004. “Insights into the ‘Healthy Immigrant Effect’: Health Status and Health Service Use of Immigrants to Canada.” Social Science & Medicine 59(8):1613–1637.
McKissick, J. C. and S. P. Kane. 2011. An Evaluation of Direct and Indirect Economic Losses Incurred by Georgia Fruit and Vegetable Producers in Spring 2011. Athens, GA: Center for Agribusiness and Economic Development, University of Georgia.
Mohanty. S. A. 2006. “Unequal Access: Immigrants and U.S. Health Care.” Immigration Policy in Focus 5(5):1–7.
Mohanty S. A., S. Woolhandler, D. U. Himmelstein, S. Pati, O. Carrasquillo, and D. H. Bor. 2005. “Health Care Expenditures of Immigrants in the United States: A Nationally Representative Analysis.” American Journal of Public Health 95(8):1431–1438.
Passel, J. S. 2015. “Share of Unauthorized Immigrant Workers in Production, Construction Jobs Fall Since 2007.” Hispanic Trends. Washington, D.C.: Pew Research Center. Available online: http://www.pewhispanic.org/2015/03/26/share-of-unauthorized-immigrant-workers-in-production-construction-jobs-falls-since-2007/
Perkins, J., and M. Youdelman. 2008. Summary of State Law Requirements Addressing Language Needs in Health Care. Washington, D.C.: National Health Law Program.
Preston, J. 2007, 5 September. “Short on Labor, Farmers in U.S. Shift to Mexico.” New York Times. Available online: http://www.nytimes.com/2007/09/05/us/05export.html .
Ruark, E. A., and A. Moinuddin. 2011. Illegal Immigration and Agribusiness: The Effect on the Agriculture Industry of Converting to a Legal Workforce. Washington, D.C.: Federation for American Immigration Reform.
Smith, J., and C. Medalia. 2014. Health Insurance in the United States: 2013 Current Population Reports, P60–250. Washington, D.C.: U.S. Census Bureau. Available online: https://www.nber.org/cps/hi/2014redesign/p60-250.pdf
Smith, R., and A. Sugimori. 2015. Undocumented Workers: Preserving Rights and Remedies after Hoffman Plastic Compounds v. NLRB. New York, NY: National Employment Law Project.
Sundaram-Stukel, R., and S.C. Deller. 2009. “Farmer Health Insurance Cooperatives: An Innovative Solution for Other Americans?” Choices 24(4).
Wells, J. 2012, 20 August. “California Farm Labor Shortage ‘Worst it’s been ever.” CNBC. Available online: http://www.cnbc.com/id/48725145
Wozniacka, G. 2013, 27 September. “Farmers Face Labor Shortages as Workers Find Other Jobs.” Associated Press. Available online: http://dnews.com/news_ap/farmers-face-labor-shortages-as-workers-find-other-jobs/article_35a6e3a9-8d05-5332-acab-982590e27be4.html
U.S. Census Bureau/U.S. Bureau of Labor Statistics. 2010. Current Population Survey, Annual Social and Economic Supplement. Washington, D.C.: U.S. Census Bureau.
U.S. Department of Agriculture. 2012. Farm Labor. Washington, D.C.: National Agricultural Statistics Service.
http://journals.sagepub.com/doi/full/10.1177/1035304617703933
https://ideas.repec.org/p/ags/aaea16/235620.html
http://ageconsearch.tind.io/record/205110

