Public health within the United States is becoming a concern not only from the perspective of rapidly expanding health care costs but also in terms of economic productivity. Obesity and other diet-related diseases are said to becoming epidemic. At the same time, in both rural and poorer urban areas, the notion of “food deserts”—geographic areas with limited access to and availability of affordable healthy foods—is gathering significant attention. While the complex relationships between poverty and health outcomes are well-documented, it is not clear if food access changes these relationships, especially in the rural United States.
The links between poverty and poor health outcomes are numerous, complex, and intertwined. Since Lyndon Johnson’s call for a “War on Poverty” in 1964 launching a new era of welfare legislation, defining and addressing poverty issues have been focal points for public policy discussions and social welfare organizations. While there is well-developed literature in urban food access and poverty, rural poverty issues have received notably less attention in both the academic research and policy arenas. This is significant since poverty rates are highest in the most urban and most rural areas of the United States. Additionally, high and persistent poverty disproportionately occurs in rural areas (Weber et al., 2005).
It is well understood by community development professionals that “place matters” in discussions of poverty, or in other words, the causes, consequences, and policy measures for addressing poverty may differ across the urban-rural continuum. If this is the case, we might then ask, “What does rural poverty look like?” Most quantitative literature defines poverty according to the official U.S. Census definition in which a family is considered poor if its annual pre-tax income (excluding non-cash benefits such as food stamps) is less than the federal poverty threshold. These thresholds vary according to household size, but have not changed substantially since the 1960s. Studies will often look at contextual or community issues affecting poverty since income is typically used as the measure for defining being poor. According to these studies, the persistent effects of poverty in rural areas may be rooted in rural households’ isolation from schools, services, social interactions, and labor-market resources. Local community dynamics affecting cross-class relations, social capital, and race may also have an effect on poverty in rural areas. Similarly, contextual research suggests that living in a rural area may increase one’s chances of being poor (Weber et al., 2005). It is important to note, however, that the current and most commonly used measure of poverty has been substantially critiqued in that it fails to adjust for changes in standards of living over time or geography, or for availability of public goods which may vary significantly between urban and rural areas.
There are numerous personal and social ills associated with poverty. One that is well documented is its relationship with health. Disparities in health outcomes based on income alone are observed across subpopulations, accounting for race, ethnicity, and education, among other social factors. In addition, a growing body of literature places these social factors, known as social determinants of health, at the root of health inequalities (Marmot, 2005). Galea et al. (2011) recently found that 133,000 deaths in the United States were attributable to individual-level poverty; 199,000 to income inequality; and 39,000 to area-level poverty. These authors go on to note that their findings suggest a need to broaden the frameworks for defining health and accompanying program and policy responses—which can include the facilitative effects on reducing the negative health impacts associated with poverty.
Rates of both diet-related chronic disease and food insecurity have increased substantially in recent decades, and low-income and rural populations are disproportionately affected. Although the rate of growth in obesity appears to be slowing, more than one-third of adults and almost 17% of adolescents were obese in 2009-2010 (Flegal et al., 2010; and Ogden et al., 2012), and the incidence and prevalence of type 2 diabetes continues to rise with nearly one-third of the population in the United States classified as having diagnosed diabetes in 2010 (U.S. Center for Disease Control, 2011). Meanwhile, in 2012, approximately 17.6 million households, or 14.5% of the U.S. population, were classified as food insecure, meaning they lack assured access to affordable, healthy foods at all times (Coleman-Jensen, Nord, and Singh, 2013).
The rise in diet-related chronic disease can be attributed to a number of factors, among them poor dietary choices, limited knowledge about nutrition, food environments characterized by deficient access to and availability of healthy foods, public policies, and social norms. While all are likely at play, there has been growing interest in the notion of “food deserts,” particularly in urban areas. The role of food deserts in understanding the relationship between poverty and health outcomes is not well understood. A central question within this small but growing literature is if access to healthier foods within the food environment alleviates the poverty and poor health relationship.
The recently popular notion of “food deserts” is gathering significant attention with regards to the role this particular food environment plays in influencing dietary behavior and health outcomes. The general premise is that these areas have limited access to supermarkets which are more likely to offer a wider variety of healthy food products at lower prices when compared to other food outlets, such as convenience stores and fast food restaurants (Ver Ploeg et al., 2009). Both urban and rural food desert census tracts in the United States have been characterized as having not only higher rates of poverty, but also greater concentrations of Latino and African-American populations. Further, residents in rural and urban food deserts tend to have lower vehicle access rates and are more likely to rely on public transportation or alternative methods of commuting when compared to other rural and urban areas (Dutko, Ver Ploeg, and Farrigan, 2012). Given that the majority of U.S. citizens are highly dependent on a vehicle for grocery shopping, access to transportation is a particularly critical factor for low-income households in rural food deserts.
Prior research attempting to document the health-related impacts of geographic areas with limited food access has yielded mixed results and has been largely centered on urban food environments. Jilcott, et al (2011) found that in rural counties, but not urban counties, obesity rates were significantly lower in areas with a higher density of farmers’ markets. Supercenters and grocery stores were also found to be inversely associated with obesity rates in both rural and urban areas. Similarly, Ahern, Brown, and Dukas (2011) found that in both rural and urban counties more convenience stores were associated with poorer health outcomes, including adjusted mortality, diabetes, and obesity rates. Variations across rural and urban counties, however, appeared when comparing healthier food retail options. In rural counties, a greater number of per capita grocery stores were associated with lower diabetes and mortality rates, but greater obesity rates. By contrast, lower obesity rates in rural counties were associated with more per capita fast-food restaurants. Adjusted mortality rates were also inversely associated with greater per capita full-service restaurants and grocery stores, and greater per capita direct farm sales.
The unexpected association between obesity and grocery store presence in rural counties has been supported, to some degree, by others investigating the relationship between obesity, fruit and vegetable consumption, and distance to the grocery store—finding no association for rural areas (Michimi and Wimberly, 2010). These contrasting findings, and lack of causal pathways, suggest the need for additional factors mitigating the relationships between diet-related disease and food environments, particularly in rural areas.
To explore the extent to which various levels of food access—“healthy” or “unhealthy”—mitigates the strong and predictive relationship between poverty and health outcomes, we examine the extent to which these variables are correlated. More specifically, we show the geographical relationships by mapping rural poverty, public health outcomes, and food access using data for non-metropolitan counties for calendar year 2010. Our analysis cannot address issues of causation, but only association.
The food access index was constructed using data available on the U.S. Department of Agriculture (USDA) Food Environment Atlas. Healthy food access measures—including grocery stores, supercenters, and farmers markets—were combined with all on a per 1,000 population basis. Unhealthy food access measures include fast food restaurants and convenience stores, also on a per 1,000 population basis. This simple measure of access to healthy foods reflects a weakness in the ecological food environment literature since access to these different types of food outlets is just one component influencing personal dietary behavior. For example, access to a full-range grocery store is generally assumed to be associated with better food access, but this simple measure does not provide any insight into the buying and eating habits of consumers, which may also be driven by personal preference, price, convenience, cooking skills, and nutrition knowledge, among others. In addition, grocery stores carry both healthy and unhealthy foods. It is clear that access to food, both healthy and unhealthy, does not ensure any particular type of eating habits and is just one component of the social-ecological factors influencing dietary behavior.
We also constructed a measure of public health reflective of the dietary behavior impact on morbidity and mortality using data from the County Health Rankings project, a collaboration between the University of Wisconsin Population Health Institute and the Robert Wood Johnson Foundation (2013). The health index consists of five variables: percent of adult obese, percent of adult diabetic, percent low-birth weight, percent fair/poor health, and years of potential life lost (premature death). Higher values of each of these metrics in the public health index are associated with poorer overall levels of health. One of the limitations to the public health data is that the data are not available for all non-metropolitan counties for every year. This means that data values may be missing for smaller, more rural counties.
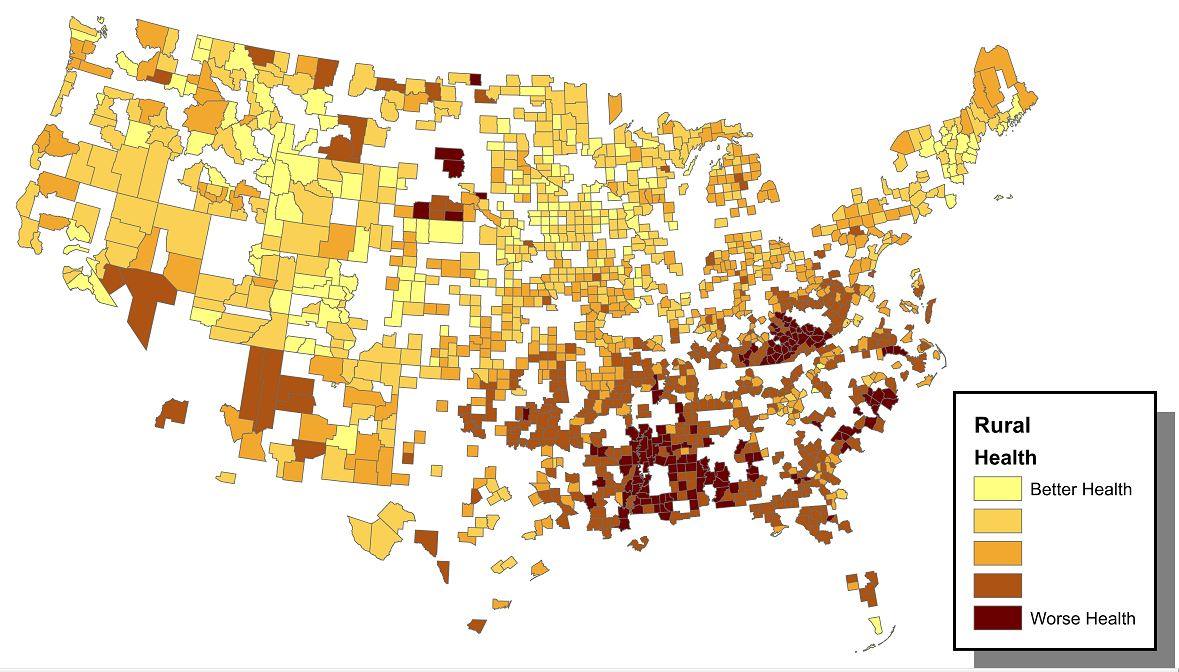
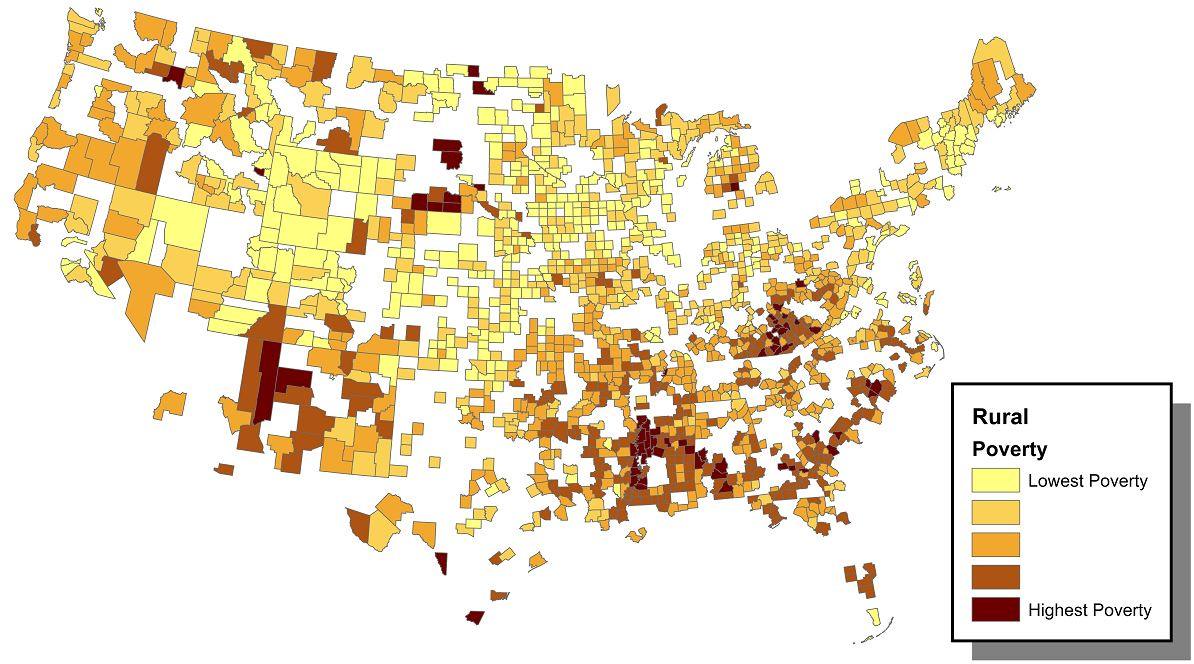
A simple mapping of the three county characteristics of central interest—rural poverty, health outcomes, and food access—are provided in Figures 1-3. There are clear spatial clusters or concentrations of high-poverty areas in the southern United States and parts of the southwest areas associated with Native American reservations. The corresponding mapping of our health index—where higher values are associated with poorer health—reveals a very similar pattern to poverty: poorer rural health is concentrated in the southern United States and lands associated with Native American tribes. Indeed, there almost appears to be a one-to-one mapping and is consistent with the strong poverty-health relationship. The mapping of food access, proxied by our simple measure, is less clear but a similar pattern to poverty and health is evident: lower access to healthy foods tends to be clustered in the southern United States and a smaller region of the southwestern United States. Better access to healthy food appears to be in the Midwest, Great Plains, and towards the Pacific Northwest. On face value, there appear to be relationships between our three variables of interest.
To further explore the relationships between poverty, health, and access to healthy foods, we used several advanced statistical techniques and found the results are generally consistent with the findings from our mapping. We generally find a strong relationship between rural poverty and health where higher poverty is associated with poorer levels of public health. We also find that higher levels of healthy food access are associated with better health.
The more important finding is that higher concentrations of poverty and healthy food access tend to be associated with better health. At the same time, lower levels of poverty coupled with lower access to healthier foods tend to be associated with worse health. What this is telling us is that promoting access to healthier foods in rural areas may help mitigate the poverty and health relationship. This is consistent with a previous study exploring the attenuating effect of food environment factors on the relationship between obesity and county-level, persistent poverty in rural areas (Bennett, Probst, and Pumkam, 2011).

There is a growing interest in understanding how access to food, particularly healthier food, impacts the poverty and health-outcome relationship. While the association between poverty and poor health has been well documented, the direct impact of healthier food environments on alleviating the negative effects of that relationship is less well understood and recognizably complex. Although an understanding of food access in urban areas is growing, there are fewer studies focused solely on rural food access. Not only are the insights from the urban food environment literature mixed, but they may not be transferable to a rural setting. Our simple discussion of the food access, poverty, and health relationships provide limited insights, but it does suggest some important questions:
A natural question centers on the effectiveness of programmatic responses to date. For example, the response to the “food deserts” literature has prompted First Lady Michelle Obama’s “Let’s Move” initiative and other non-profits to call for the introduction of supermarkets in areas of limited access and availability of affordable, healthy foods. In addition, growing attention towards local and regional food systems have prompted interest in exploring the role of direct-to-consumer food access initiatives such as farmers’ markets and community-supported agriculture. However, citing the complex market and behavioral economic forces behind consumer shopping behaviors, others have criticized these initiatives. Low-income households tend to shop where food prices are lowest, when possible, and purchases at convenience stores make up a small percentage of overall total food expenditures. Critics, therefore, question whether these programs aimed at promoting access to healthy foods fall into the “if you build it, they will come” trap?
An additional difficulty with outlining policy options for looking at “food deserts” within the context of rural poverty and health is that the research foundation is weak. While there has been a growing urban-focused literature, the scientific rigor of much of this research is lacking. Much is descriptive and based on limited case studies—almost anecdotal story-telling—making it difficult to draw generalizations. While the limited evidence suggests that promoting the access of healthier foods in rural areas could be a potential strategy to mediate poverty’s link to poor health, more work is required before effective policies can be crafted.
Ahern, M., C. Brown, and S. Dukas. (2011). A national study of the association between food environments and county-level health outcomes Journal of Rural Health 27:367-379.
Bennett, K.J., J.C. Probst, and C. Pumkam. (2011). Obesity among working age adults: The role of county-level persistent poverty in rural disparities. Health and Place 17:1174-1181.
Coleman-Jensen, A., M. Nord, and A. Singh. (2013). Household food security in the United States in 2012. U.S. Department of Agriculture, Economic Research Service, ERR-155.
Dutko, P., M. Ver Ploeg, and T. Farrigan. (2012). Characteristics and influential factors of food deserts. U.S. Department of Agriculture, Economic Research Service, ERR-1401.
Flegal, K.M., M.D. Carroll, C.L. Ogden and L.R. Curtin. (2010). Prevalence and trends in obesity among U.S. adults, 1999–2008. Journal of the American Medical Association 303:235–41.
Galea, S., M. Tracy, K. Hoggatt, C. DiMaggio, and A. Carpatti. (2011). Estimated deaths attributable to social factors in the United States. American Journal of Public Health 101:1456-1465.
Jillcot, S.B., T. Keyserling, T. Crawford, J.T. McGuirt, and A.S. Ammerman. (2011). Examining association among obesity and per capita farmers’ markets, grocery stores/supermarkets, and supercenters in U.S. counties. Journal of the American Dietetic Association 111:567-572.
Marmot, M. (2005). Social determinants of health inequalities. The Lancet 365:1099-104.
Michimi, A. and M.C. Wimberly. (2010). Associations of supermarket accessibility with obesity and fruit and vegetable consumption in the conterminous United States. International Journal of Health Geographics 9:49. Available online: http://www.ij-healthgeographics.com/content/9/1/49
Ogden C.L., M.D. Carroll, B.K. Kit, and K.M. Flegal. (2012). Prevalence of obesity in the United States, 2009-2010. National Center for Health Statistics Data Brief, No. 82. Hyattsville, Md.
Robert Wood Johnson Foundation and the University of Wisconsin Population Health Institute. (2013). County health rankings and roadmaps. University of Wisconsin-Madison. Available online: http://www.countyhealthrankings.org/rankings/data
Rural Poverty Research Center. (2004). Synthesis of the RUPRI Rural Poverty Research Conference: Place matters: addressing rural poverty. Rural Policy Research Institute, University of Missouri. April. Available online: http://www.rupri.org/Forms/synthesis.pdf
U.S. Centers for Disease Control and Prevention. (2011). National diabetes fact sheet: national estimates and general information on diabetes and pre-diabetes in the United States. U.S. Department of Health and Human Services: Atlanta, Ga.
U.S. Department of Agriculture. (2013). Food environment atlas. Economic Research Service. Available online: http://www.ers.usda.gov/data-products/food-environment-atlas.aspx.
U.S. Department of Agriculture. (2014). Rural poverty and well being. Economic Research Service. Available online: http://www.ers.usda.gov/topics/rural-economy-population/rural-poverty-well-being/poverty-overview.aspx#.UyMr4rQXcqU.
Ver Ploeg, M., V. Berneman, T. Farrigan, K. Hamrick, D. Hopkins, P. Kaufman, B-H. Lin, M. Nord, T.A. Smith, R. Williams, K. Kinnison, C. Olander, A. Singh, and E. Tuckermanty. (2009). Access to affordable and nutritious food-measuring and understanding food deserts and their consequences: Report to Congress. AP-036, U.S. Department of Agriculture, Economic Research Service. Available online: http://ers.usda.gov/publications/ap-administrative-publication/ap-036.aspx#.U7X277HSikc.
Weber, B., L. Jensen, K. Miller, J. Mosley, and M. Fisher. (2005). A critical review of rural poverty literature: is there truly a rural effect? Institute for Research on Poverty. Discussion Paper No. 1309-05. April. University of Wisconsin-Madison. Available online: http://www.irp.wisc.edu/publications/dps/pdfs/dp130905.pdf .

