Since the first cases of COVID-19 appeared in January 2020 in the United States, the pandemic’s death toll has risen sharply in the country, surpassing 540,000 deaths as of March 19, 2021, which is more than the number of Americans who died in World War II (Sergent and Padilla, 2021). Initially, the incidence of COVID-19 (cases per 100,000 people) was greater in metro areas than in nonmetro areas of the country,[1] but this trend started to change after October 2020, when the cumulative cases per 100,000 in nonmetro areas started to surpass the cases in metro areas. By December 2020, nonmetro areas recorded 4,500 cumulative cases per 100,000 while metro areas recorded 4,000 cases per 100,000 (ERS “COVID-19 Pandemic”, 2020). Starting August 2020, COVID-19-related deaths (per 100,000) in nonmetro areas also started to surpass that of metro areas and so did the weekly rate of new infections (Murphy and Marema, 2021; Marema, 2021).
For several reasons, rural communities may be particularly vulnerable to the COVID-19 pandemic: aging population, greater share of the population with underlying medical conditions, less access to health care services, higher unemployment rates, labor-intensive workforce that requires physical presence at work, longer commutes to work, and distance to medical services and facilities (Ajilore and Willingham, 2020; Dobis and McGranahan, 2021; Marema, 2021; ERS “Rural America”, 2020; Vestal, 2020; Zaller, 2020). For example, 17% of the nonmetro population was at least 65 years old in 2012–2016, compared to only 13.8% in metro areas (ERS “Rural America at a Glance”, 2020; Smith and Trevelyan, 2019). Probably the biggest challenge is the lack of access to hospitals and health facilities, let alone intensive care units that can treat acute COVID-19 cases (Ajilore, 2020; Dobis and McGranahan, 2021). According to the USDA Economic Research Service (ERS “Rural America at a Glance”, 2020), in 2016–2017, the United States had 116 counties without a medical clinic or hospital, 97 (83%) of which were nonmetro counties. Additionally, 77% of counties without an intensive care unit were also in nonmetro counties. These long-running health and economic inequities in rural areas remain a key focus of federal rural policy.
The main goal of the USDA’s Rural Development (RD) mission area is to advance rural prosperity and improve quality of life in rural America. The RD offers loans, loan guarantees, grants, and technical assistance programs to accomplish this goal, and there are several programs targeted toward improving rural health. The Community Facilities (CF) Program is one of the major RD programs, and it finances community facilities and infrastructure development in rural areas including health care systems and related services and amenities. Although the CF Program was instituted in the late 1960s, there have been no published studies on the program. In this short paper, we detail CF investments to health facilities for the period between 2016 and 2020 and associated COVID-19 conditions at the county level. We also investigate whether CF health-funded counties had a lower COVID-19 death rate compared to a similar group of counties that did not receive CF health funds during the same period. Our analysis shows that nonmetro counties had higher COVID-19 case and death rates than metro areas, and high-poverty counties had higher COVID-19 case and death rates than low-poverty counties. Regardless of rurality or poverty level, CF health-funded counties had lower COVID-19 case and death rates. Results of the impact analysis show that, on average, CF health-funded counties had 0.22 percentage points lower COVID-19-related deaths (per case) in nonmetro areas compared to a group of similar counties that did not receive health-related CF investments, implying 220 fewer deaths per 100,000 cases in CF health-funded counties. These impacts are even stronger for remote, nonmetro counties that received CF health funds where the COVID-19 deaths per case was 0.55 percentage points lower compared to the nonrecipient group of counties, implying 550 fewer deaths per 100,000 cases in CF health-funded counties.
The Community Facilities Program offers grants and loans programs for rural America to improve facilities and infrastructure, including hospitals, health care clinics, assisted living facilities, rehabilitation centers, public buildings, schools, community-based facilities, and fire and rescue stations. The program also covers costs for land acquisition, professional fees, purchase of equipment, and technical assistance (USDA RD, 2021). We obtained administrative program data from Rural Housing Services (RHS) of the USDA Rural Development and use project descriptions and North American Industry Classification System (NAICS) codes to select health-related investments. We focus on CF health-related grants and loans obligated for the period between 2016 and 2020. During this period, 508 counties, about 16% of U.S. counties, received $3.6 billion in CF health-related investments (Table 1). Communities—counties, small towns, or villages—with less than 20,000 population are eligible for all CF programs.[2] Priority is also given to low-income communities.[3] Due to this subcounty population eligibility criterion, a small village or a town inside a metro county can also qualify for CF program.
| RUCC 2013 | Total No. of Counties | No. of Counties Received CF Health | Percentage of Counties Received CF Health $ | Percentage of CF_Health Investments to Each RUCC | CF_Health Investments Total, 2016-2020 ($millions) | Total Population 2015 ACS 5 YR (millions) |
| 1 | 472 | 23 | 7% | 6% | $217 | 176 |
| 2 | 394 | 50 | 13% | 11% | $390 | 68 |
| 3 | 360 | 37 | 10% | 7% | $256 | 29 |
| 4 | 217 | 35 | 16% | 7% | $267 | 14 |
| 5 | 92 | 18 | 20% | 5% | $168 | 5 |
| 6 | 597 | 108 | 18% | 23% | $837 | 15 |
| 7 | 434 | 111 | 26% | 31% | $1.12 | 8 |
| 8 | 220 | 32 | 15% | 2% | $67 | 2 |
| 9 | 425 | 83 | 20% | 8% | $278 | 3 |
| U.S. | 3220 | 508 | 16% | 100% | $3.60 billion | 320 |
Source: ERS, RUCC 2013 (2013); Census Bureau, 2015 ACS 5 YR Estimates; CF Program data by USDA RD Data Analytics Division (2020). COVID-19 data by The New York Times and Chetty et al. (2020) Economic Opportunity Insights Economic Tracker.
Source: Authors’ calculations using USDA RD CF Program
Data, COVID-19 data by The New York Times and Chetty et al.
(2020) Economic Opportunity Insights Economic Tracker.
Source: ERS, RUCC (2013); Census Bureau, 2015 ACS 5 YR
Estimates; CF Program data by USDA RD Data Analytics
(2020). COVID-19 data by The New York Times and Chetty
et al. (2020) Economic Opportunity Insights Economic Tracker.
Source: Economic Innovation Group, Distressed Community
Index 2013; ERS, RUCC 2013; Census Bureau, 2015 ACS
5 YR Estimates; CF Program data by USDA RD Data Analytics
(2020). COVID-19 data by The New York Times and Chetty
et al. (2020), Economic Opportunity Insights Economic Tracker.
In this section, we briefly investigate the incidence of health-related investments of the CF Program in relation to COVID-19 pandemic, identifying areas and populations benefiting from the programs and comparing those to eligible areas and populations not benefiting from the program. We group the counties into metro and nonmetro areas using the Rural–Urban Continuum Codes (RUCC) for 2013 developed by the USDA Economic Research Service,[4] which classifies counties into three metro categories and six nonmetro categories based on population size and proximity to urban centers. Eligible communities within metro counties (RUCC 1–3) received 24% of CF health-related funding and nonmetro counties (RUCC 4–9) received 76% of such funding between 2016 and 2020. Counties in RUCC 6 and 7 classifications (nonmetro counties with an urban population of 2,500–19,999) are the closest to the maximum size threshold for CF population eligibility, and these counties received a larger portion of the funding, 23% and 31% respectively. Counties in RUCCs 8 and 9 classifications are completely rural, with urban populations of less than 2,500, and they received 2% and 8% of health-related funding, respectively.
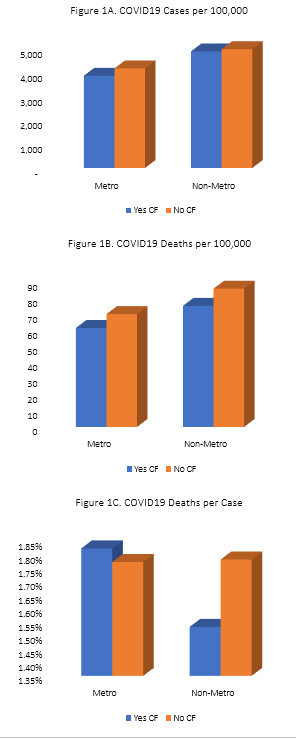
Next, we examine the COVID-19-related health outcomes in the counties that received CF health investments using COVID-19 cases and deaths per 100,000 as measures for COVID-19 outcomes and data from The New York Times and the COVID-19 tracking project by Chetty et al. (2020).[5] We also use deaths per case as a percentage for comparison purposes. Figure 1 shows COVID-19 cases and deaths comparison between nonrecipient counties and recipient counties of CF health investments, depending on whether they are metro or nonmetro. In general, cases per 100,000, deaths per 100,000, and death rate per case are lower in counties that received CF health investments. CF recipient counties reported 4,623 cases per 100,000, while nonrecipient counties reported 4,645 cases per 100,000 from January to November 2020 (Figure 1A). In metro areas, counties with CF health investments reported 308 fewer cases per 100,000 on average. In nonmetro areas, CF recipient counties recorded 90 fewer cases per 100,000 on average compared to nonrecipient counties for the same period. As for COVID-19-related deaths, CF recipient counties reported 72 deaths per 100,000 people while nonrecipient counties reported 79 deaths per 100,000 population as of November 2020 (Figure 1B). Nonmetro CF recipient counties recorded 10 fewer COVID-19 deaths per 100,000 compared to nonmetro, nonrecipient counties (Figure 1B). In nonmetro CF recipient counties, 1.53% of cases resulted in death; the corresponding number in nonmetro, nonrecipient counties was 1.78% (Figure 1C).
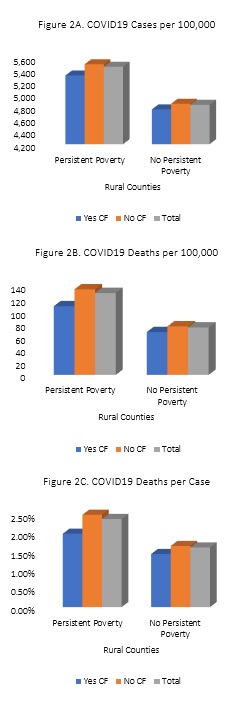
The Community Facilities Program gives priority to low-income communities, which have been disproportionally affected by the pandemic (CBS News, 2020; UCLA Public Health, 2020). In this section, we group nonmetro counties based on poverty and distress levels using two measures: persistent poverty and Distressed Community Index (Economic Innovation Group, 2020). Persistent poverty counties are defined as those that had 20% or more of the county population living under established poverty-level household incomes in each of the last three decades (based on decennial census). We find that regardless of whether a county received CF health investments, persistently poor counties suffer more from COVID-19 in rural America. On average, nonmetro counties with persistent poverty reported 610 more COVID-19 cases (Figure 2A) and 54 more COVID-19-related deaths per 100,000 (Figure 2B). However, the persistent-poverty counties with CF health investments had overall better COVID-19 outcomes than those without CF investments. In nonmetro areas, 22% of counties with persistent poverty received CF health investments between 2016 and 2020 and 19% of nonpersistent-poverty counties received such investments. The nonmetro persistent-poverty counties that received CF investments reported 180 fewer cases (Figure 2A) and 26 fewer deaths (per 100,000 population) (Figure 2B) compared to the nonmetro persistent-poverty counties that did not receive CF investments. Similarly, persistent poverty counties with CF health investments in nonmetro areas reported 0.51% fewer deaths per case compared to persistent poverty counties without CF investments (Figure 2C).
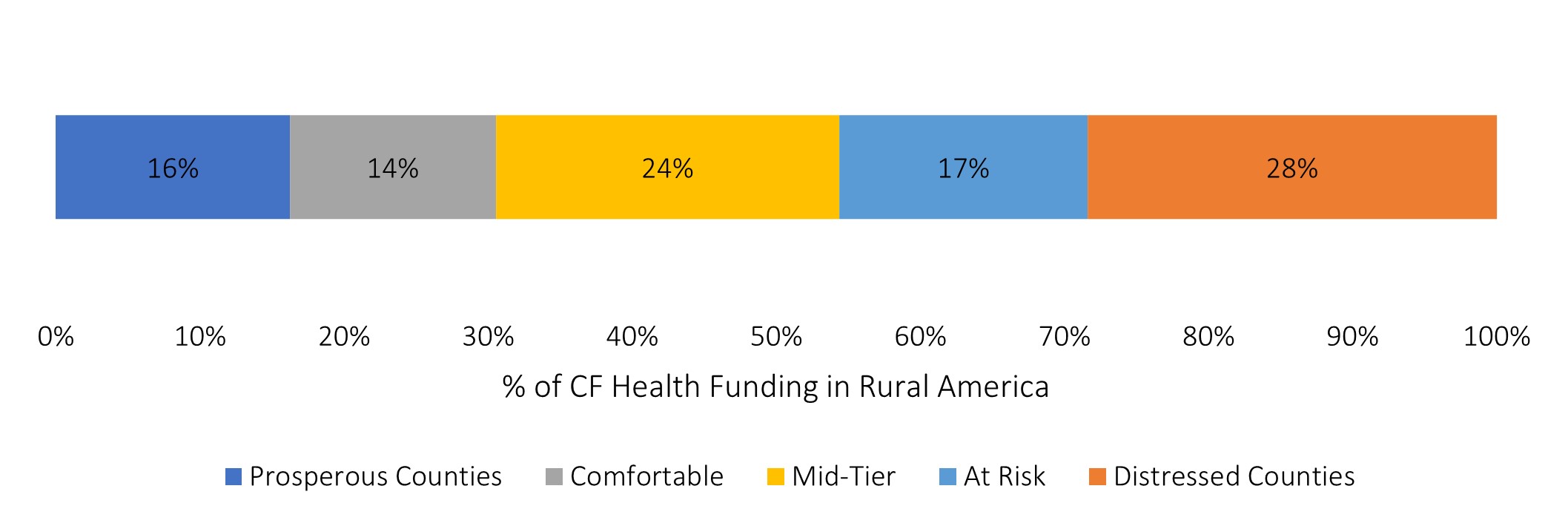
The Distressed Community Index (DCI) developed by the Economic Innovation Group (2020) encompasses not only a county’s poverty level but also other socioeconomic conditions such as education, unemployment, adults not working, housing conditions, income, and changes in employment and number of local businesses. The DCI ranges from 0 to 100 (0 being the most prosperous and 100 the most distressed) and classifies counties into five categories: prosperous (DCI < 20); comfortable (20 < DCI < 40); mid-tier (40 < DCI < 60); at-risk (60 < DCI < 80); and distressed (DCI > 80). The counties classified as mid-tier, at-risk, and distressed together received more than half of the total CF health investments allocated to nonmetro counties between 2016 and 2020 (Figure 3). Figure 3 also shows that distressed counties received the largest proportion (28%) of total CF health investments.
We find that regardless of whether counties received CF health investments, distressed areas experienced more COVID-19 cases and deaths in rural America (Table 2). Distressed counties reported 452 more cases per 100,000 than prosperous counties. Looking at death rates, distressed counties reported 112 deaths per 100,000 and 2.27% deaths per case, while prosperous counties reported 62 deaths per 100,000 and 1.12% deaths per case. Nevertheless, counties that received CF health investments generally fared better in both cases per 100,000 and death rates (per 100,000 and per case) (Table 2). Among distressed counties, CF recipient counties reported 354 fewer COVID-19 cases and 17 fewer deaths per 100,000 on average than nonrecipients. In terms of death per cases, distressed CF recipient counties reported 2.02% of deaths and distressed nonrecipient counties reported 2.33% of deaths. However, among prosperous counties, CF recipient counties reported 48 more cases per 100,000 than nonrecipients; interestingly, prosperous CF-recipient counties reported 19 fewer deaths per 100,000 than the prosperous nonrecipient counties. In terms of cases resulting in deaths, prosperous CF-recipient counties reported a 0.93% death rate while prosperous nonrecipient counties reported a 1.18% death rate.
In summary, the descriptive analysis above shows the vulnerability of rural America to the pandemic, regardless of a county’s level of rurality, poverty, or distress. The analysis also confirms that poorer and more distressed counties are more vulnerable to the pandemic. Overall, nonmetro counties that received CF health investments seemed to perform better on average with respect to COVID-19 outcomes, regardless of the level of poverty, level of distress, or remoteness. However, we cannot infer from this descriptive analysis whether the health investments from the CF actually had any impact on lowering COVID-19-related outcomes such as deaths because CF investments were not randomly distributed among counties. In the rest of the paper, we undertake a brief impact analysis to examine whether the lower COVID-19 death rates in the counties that received CF health investments can be attributed to the CF programs.
In this section, we estimate whether CF health related investments had an impact on COVID-19 death rates in recipient counties. We conjecture that the counties that received CF investments for health care, nursing, and private physicians care facilities, and emergency response equipment were better prepared to meet the COVID-19 pandemic challenges, which would therefore result in a lower COVID-19 death rate. To study the impact, we compare the COVID-19 death rate of nonrecipient counties to that of funding recipient counties. However, CF recipient counties and nonrecipient counties can differ in many ways, making it difficult to compare the outcomes between the two groups of counties. This situation motivates us to use matching techniques to select a comparison group of counties from non-CF funded counties based on economic, demographic, and housing characteristics.
We use several sociodemographic and economic variables measured before our study period to create a matched comparison group of counties. These variables include CF program eligible population data from USDA-RD data and total population, race, ethnicity, age (people over 65), gender, people without health insurance, and median household income from 2015 American Community Survey (ACS) data. We also control for county-level overall death rates[6] (excluding accidental deaths) for the five-year period before 2016 to ensure that the matched comparison group has similar death rates to that of funding recipient group before the period considered for impacts. Additionally, we control for the rural–urban hierarchy using the Rural–Urban Continuum Codes (RUCC) and make sure that each recipient county in a particular RUCC code is matched with a nonrecipient county in the same RUCC code. The group of funding recipients consists of 505 counties (out of 3,142) that received CF health investments at least once during the period considered. The impact of CF investments on COVID-19 death rate is estimated by taking the difference in death rate between matched recipient and nonrecipient counties.
| Average COVID-19 Cases per 100,000 | Average COVID-19 Deaths per 100,000 | Average COVID-19 Deaths per Case | ||||
| CF Health Investments | Nonmetro Most Distressed | Non Metro Prosperous Counties | Nonmetro Most Distressed | Nonmetro Prosperous Counties | Nonmetro Most Distressed | Nonmetro Prosperous Counties |
| Yes | 4,691 | 5,464 | 98 | 47 | 2.02% | 0.93% |
| No | 5,045 | 5,416 | 115 | 66 | 2.33% | 1.18% |
| Total | 4,974 | 5,426 | 112 | 62 | 2.27% | 1.12% |
Source: Economic Innovation Group, Distressed Community Index 2013 (2020); ERS, RUCC 2013; Census Bureau, 2015 ACS 5 YR Estimates; CF Program data by USDA RD Data Analytics (2020). COVID-19 data by The New York Times and Chetty et al. (2020) Economic Opportunity Insights Economic Tracker.
| CF Health Investments Yes (1) or No (0) | Average Treatment Effect Coefficient |
| All counties (275 matched) | -0.0012 (0.0011) |
| Metro counties (61 matched) | -0.0001 (0.0022) |
| Nonmetro counties (214 matched) | -0.0022* (0.0013) |
| Rural, not adjacent to metro (119 matched) | -0.0055*** (0.0017) |
| Rural, adjacent to metro (95 matched) | 0.0007 (0.0014) |
| Persistent poverty counties (84 matched) | -0.0048* (0.0029) |
| No persistent poverty counties (466 matched) | -0.0018+ (0.0013) |
| Not Excluded Group with CF-Investments, 2010-2015 | |
| All counties (501 matched) | -0.0003 (0.0007) |
| Metro counties (116 matched) | 0.0009 (0.0014) |
| Nonmetro counties (385 matched) | -0.0014 (0.0009) |
| Rural, not adjacent to metro (211 matched) | -0.0023* (0.0013) |
| Rural, adjacent to metro (174 matched) | 0.0006 (0.0011) |
Note: *** indicates |p|<.01; ** indicates |p|<.05; * indicates |p|<.10; + indicates |p|<.20. Statistical
significances are based on two-tailed tests.
Source: ERS, RUCC 2013; Census Bureau, 2015 ACS 5 YR Estimates; CF Program data by
USDA RD Data Analytics (2020). COVID-19 data by The New York Times and Chetty et al.
(2020) Economic Opportunity Insights Economic Tracker.
The impact results reported in Table 3 from the matching analysis show that nonmetro counties with CF health investments had fewer COVID-19 deaths per case.[7] Results for the all-counties model show that the CF health investments recipient counties had a lower death rate compared to nonrecipient counties. However, the coefficient estimate is imprecise, and we cannot rule out that there is no effect of CF investments on COVID-19 death rates. Results for all nonmetro counties and remote nonmetro (nonmetro, not adjacent to metro) samples suggest that the seemingly lower death rate in investments recipient counties in the all counties model is mainly due to statistically significant lower death rate in recipient counties in these subsamples. For all nonmetro counties, having CF health investments could lower deaths per case by 0.22 percentage points. This could mean an additional two people would have survived from COVID-19 for every 1,000 COVID-19 cases, or additional 220 people would have survived for every 100,000 cases due to CF health investments. For the remote nonmetro (not adjacent to metro) county sample, the estimated impact is 0.55 percentage points fewer deaths per case. This could mean additional 550 people would have survived from COVID-19 for every 100,000 cases due to CF health investments in this group of counties. We also estimate the impact by classifying counties based on persistent poverty status. For counties experiencing persistent poverty, the estimated impact is statistically significant and shows a decrease of deaths per case by 0.48 percentage points in a county that received CF health investments. For counties without persistent poverty, CF health-funded counties experienced a 0.18-percentage-point decrease in deaths per case, but this effect is only marginally statistically significant.
We analyze the USDA Community Facilities Program’s assistance to health-care related services and facilities for the period between 2016 and 2020 and examine whether the counties that received investments had fewer case counts/rates and death counts/rates compared to the counties that did not have CF health investments. Regardless of the level of rurality, poverty, or distress, rural America is more vulnerable to the COVID-19 pandemic. The analysis also confirms that poorer and more distressed counties are more vulnerable to the pandemic. However, nonmetro counties that received CF health investments seemed to perform better on average with respect to COVID-19 outcomes, regardless of the level of poverty, level of distress, or remoteness. After a descriptive analysis of the program, we present an impact analysis of CF health investments on COVID-19-related deaths, measured in deaths per case. We find that counties that received CF health investments between 2016 and 2020 had fewer deaths per case than counties that did not receive CF health investments in general. We find this effect to be statistically significant among all CF funded nonmetro counties, and even more so in nonmetro remote counties.
However, findings presented in this paper should be viewed with caution. The descriptive analysis presented in the first part of the paper shows some relationships with COVID-19-related outcomes and CF health investments, but this part of the analysis is not meant to draw any inference that CF investments had any impact on COVID-19-related outcomes. Findings presented in the second part of the paper are meant to draw causal inferences, but they should be subject to several caveats. First, this analysis was conducted at the county level even though the CF investments is targeted toward health-related facilities in counties. A more thorough analysis would have been conducted at the facility level, but we do not have access to COVID-19-related outcomes and other facility level covariates that would be required for such an analysis. Second, even though we ensured that our matched control group was similar to the treated group of counties in terms of observed covariates, there could be other, unobserved factors that could affect a county’s treatment status. The existence of these unobserved factors could lead to bias in findings. Third, it is possible that the health facilities that received CF investments were able to obtain additional investments for the same reasons they were able to secure investments from the CF program and therefore any positive effect of the program on recipient counties could be obscured by other investment programs in these counties.
Ajilore, O. 2020a, July 27. “Congress Must Help Rural America Respond to the Coronavirus.” Center for American Progress. Available online: https://www.americanprogress.org/issues/economy/reports/2020/07/27/488129/congress-must-help-rural-america-respond-coronavirus/.
Ajilore, O.. 2020b, May 12. “The Coronavirus May Accelerate the Demise of Rural America.” Inside Sources. Available online: https://insidesources.com/the-coronavirus-may-accelerate-the-demise-of-rural-america/.
Ajilore, O., and Z. Willingham. 2020, March 5. “Rural Americans Are Vulnerable to the Coronavirus.” Center for American Progress. Available online: https://www.americanprogress.org/issues/economy/news/2020/03/05/481340/rural-communities-vulnerable-coronavirus/.
Ashraf, B. N. 2020. “Economic Impact of Government Interventions during the COVID-19 Pandemic: International Evidence from Financial Markets.” Journal of Behavioral and Experimental Finance 27: 100371.
CBS News. 2020, November 18. “Study Shows Low-Income LA Neighborhoods Are Most at Risk of COVID-19.” CBS Los Angeles. Available online: https://losangeles.cbslocal.com/2020/11/18/study-shows-low-income-la-neighborhoods-are-most-at-risk-of-covid-19/.
Chetty, R., J. Friedman, N. Hendren, M. Stepner, and the Opportunity Insights Team. 2020. “The Economic Impacts of COVID-19: Evidence from a New Public Database Built Using Private Sector Data.” Available online: https://opportunityinsights.org/wp-content/uploads/2020/05/tracker_paper.pdf.
Cromartie, J., E.A. Dobis, T. Krumel, D. McGranahan, and J. Pender. 2020. Rural America at a Glance: 2020 Edition. Washington, DC: U.S. Department of Agriculture, Economic Research Service, Economic Information Bulletin, EB-221, December.
Dobis, E.A., and D. McGranahan. 2021, February. “Rural Residents Appear to be More Vulnerable to Serious Infection or Death from Coronavirus COVID-19.” Amber Waves.
Economic Innovation Group. 2021. Distressed Community Index 2007 and 2013. Available online: https://eig.org/dci/get-the-data.
Marema, T. 2021, January 6. “Rural Hospitals Have a Greater Percentage of Patients with COVID-19.” Daily Yonder. Available online: https://dailyyonder.com/rural-hospitals-have-a-greater-percentage-of-patients-with-covid-19/2021/01/06/?utm_source=newsletter&utm_medium=email&utm_campaign=01-06-2020&utm_medium=email&mc_cid=3b9efb008f&mc_eid=3a8e6635eb
Murphy, T., and T. Marema. 2021, January 26. “Rate of New Infections, Deaths Declines in Rural Counties.” Daily Yonder. Available online: https://dailyyonder.com/rate-of-new-infections-deaths-declines-in-rural-counties/2021/01/26/.
National Association of Counties. 2020. “Analysis of the Fiscal Impact of COVID-19 on County Finances.” Available online: https://www.naco.org/resources/analysis-fiscal-impact-covid-19-county-finances.
The New York Times. 2020. “Coronavirus (Covid-19) Data in the United States.” [Data set]. Available online: https://github.com/nytimes/covid-19-data [Accessed December 1, 2020].
Sergent, J., and R. Padilla. January 19, 2021. “Americans Dying Faster of COVID-19 Than Our Soldiers Did in WWII.” USA Today.
Smith, A.S., and E. Trevelyan. 2019. “In Some States, More Than Half of Older Residents Live in Rural Areas.” Washington, DC: U.S. Census Bureau. Available online: https://www.census.gov/library/stories/2019/10/older-population-in-rural-america.html.
UCLA Public Health. 2020. “UCLA Model Identifies Neighborhoods That Should Have Priority for Vaccine, Other COVID-19 Help.” Available online: https://ph.ucla.edu/news/press-release/2020/nov/ucla-model-identifies-neighborhoods-should-have-priority-vaccine-other.
U.S. Census Bureau. 2015 ACS 5 Year Estimates. [Data set]. Available online: https://data.census.gov/.
U.S. Department of Agriculture. 2020. The COVID-19 Pandemic and Rural America. Washington, DC: U.S. Department of Agriculture, Economic Research Service. Available online: https://www.ers.usda.gov/covid-19/rural-america/
Economic Research Service. 2020. April 13. “COVID-19 and Rural Communities Analysis.”
U.S. Department of Agriculture. 2021. “Community Facilities Direct Loan & Grant Program.”
Washington, DC. Available online: https://www.rd.usda.gov/programs-services/community-facilities-direct-loan-grant-program
U.S. Department of Agriculture. Economic Research Service. 2013. “Rural Urban Continuum
Codes.” Washington, DC. [Data set]. Available online: https://www.ers.usda.gov/data-products/rural-urban-continuum-codes/
U.S. Department of Agriculture Rural Development. Innovation Center, Data Analytics Division.
2020. Community Facilities Program data. [Data set].
Vestal, C. 2020, October 20. “COVID-19 Patients Swamp Rural Hospitals.” [Blog post]. Stateline. Available online: https://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2020/10/20/covid-19-patients-swamp-rural-hospitals
Zaller, N.D., and G. Pro. 2020, November 11. “Is Low Mask Wearing in Rural Communities a Sign of Poor Health Messaging?” STAT. Available online: https://www.statnews.com/2020/11/11/low-mask-wearing-rural-communities-poor-health-messaging/.
[1] USDA Economic Research Service (ERS) rural–urban continuum codes (RUCC) were used to classify counties as metro/urban (codes 1–3) and nonmetro/rural (codes 4–9). These codes include nine categories: large metro areas (counties in metro areas of 1 million or more population, RUCC = 1), medium metro areas (in metro areas of 250,000 to 1 million population, RUCC = 2), small metro areas (in metro areas of 50,000 to 250,000 population, RUCC = 3), nonmetro counties with an urban population of 20,000–49,999 (adjacent or nonadjacent to a metro area, RUCC = 4 or 5), nonmetro counties with an urban population of 2,500–19,999 (adjacent or nonadjacent to a metro area, RUCC = 6 or 7), and nonmetro counties with an urban population of less than 2,500 or completely rural (adjacent or nonadjacent to a metro area, RUCC = 8 or 9). See https://www.ers.usda.gov/data-products/rural-urban-continuum-codes.aspx.
[2] Population eligibility is the same for all except for the Guaranteed Loans program and Technical Assistance Training program, which use population less than 50,000 as the cutoff.
[3] Different programs have different income eligibility requirements. The CF direct loan and grants program, which is the biggest program in terms of investments, has a priority point system based on “population, median household income for small communities with a population of 5,500 or less and low-income communities with a median household income below 80% of the state nonmetropolitan median household income.” (U.S. Department of Agriculture, 2021).
[4] RUCC codes 1, 2, and 3 are considered “metro,” and RUCC codes 4, 5, 6, 7, 8, and 9 are considered “nonmetro” or rural.
[5] See https://tracktherecovery.org/. Case counts and death counts are cumulative as of November 30, 2020, data accessed on December 12, 2020.
[6] We use data from the Centers for Disease Control and Prevention and age-adjusted death rate of age 15 years or older for underlying cause of deaths except accidental causes. Centers for Disease Control and Prevention, National Center for Health Statistics. Underlying Cause of Death 1999-2019 on CDC WONDER Online Database, released in 2020. Data are from the Multiple Cause of Death Files, 1999–2019, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Co-Operative Program. Accessed at http://wonder.cdc.gov/ucd-icd10.html on January 24, 2021.
[7] We remove counties that received CF health investments between 2010 and 2016 from the control group of counties prior to matching to reduce potential bias. We test the robustness of this exclusion in another set of matching by including them in the control group and calculating the impact. This set of results show that they approximate to those with exclusion but less robust statistically due to the potential inclusion of treated counties in the control group and creating a bias.

