

Before the 1970s, obesity prevalence—body mass index (BMI) of 30 or greater—was creeping upward at a relatively slow rate (Flegal, 1996). However, between 1976 and 2005, the prevalence of obesity increased dramatically (Ogden et al. 2007). According to the National Health and Nutrition Examination Survey (NHANES), obesity prevalence in 2007-2008 was 32.2% and 35.5% among adult males and females, respectively, representing more than a 100% increase from 1976-1980 and a 50% increase from 1988-1994 (Flegal et al. 2010).
Since 2003-2004, obesity prevalence may be leveling off for some adult population subsets. However, this is not the case for the heaviest subset of obese individuals. Grade III obesity (BMI of 40 or greater) was extremely rare before the early 1970s but has since increased at a faster rate than obesity in general (Ogden et al. 2007). Roughly 5% of adults can now be classified as severely obese. These figures are alarming because of the numerous health conditions associated with obesity, including but not limited to cardiovascular disease, type 2 diabetes mellitus, osteoarthritis, several types of cancers, dementia, and others (Must et al. 1999; Field et al. 2001). Moreover, even among obese individuals, the likelihood of these conditions occurring rises with increasing BMI. Similar trends are now seen among children and adolescents. Diseases previously thought to be found only among adults, such as diabetes, have become more common among youth in the past 15 years (Pinhas-Hamiel and Zeitler, 2007).
Because of the health consequences resulting from excess weight, the increase in obesity prevalence has profound economic consequences on employers, insurers, and government. Not only are employers and government finding it increasingly difficult to finance the high costs of obesity-related medical treatments, but also obese individuals are more likely to be absent from work and be less productive while on the job—termed presenteeism, further adversely affecting firm profitability. In this article, we present the most recent estimates available in the literature of the per capita and aggregate direct and indirect costs of obesity from an annual and lifetime perspective. We then discuss the implications of these costs for government and employers, the two groups that finance the majority of health expenditures.
Compared to normal weight individuals having a BMI between 20 and 24.9, it is estimated that Grade I obese adults with BMI between 30 and 34.9, and Grade II obese adults with BMI between 35 and 39.9, have 14% and 25% more physician visits, respectively than normal weight adults (Quesenberry, Caan, and Jacobson, 1998). Thompson et al. (2001) also found that obese adults have 48% more inpatient days per year and 1.8 times more pharmacy dispenses, including six times the number of dispenses for diabetes medications and 3.4 times the number of dispenses for cardiovascular medications.
Increased healthcare utilization among obese individuals logically results in increased annual medical expenditures. Several studies have quantified the increase in annual medical spending for obese persons. Sturm (2002) used nationally representative data to show that obesity was associated with a 35% increase in inpatient and outpatient spending and a 77% increase in prescription medication expenditures. In the most comprehensive analysis to date, Finkelstein et al. (2009) found that obesity increases per capita inpatient expenditures by 45.5%, outpatient and physician office expenditures by 26.9%, and prescription drug expenditures by 80.4% compared with normal weight expenditures. They then combined the per capita expenditure estimates with obesity prevalence data to present estimates of the costs of obesity as a percentage of total health care spending separately by payer and by type of service.
Focusing on total payments, the estimates indicate that 8.5% of Medicare expenditures, 11.8% of Medicaid expenditures, and 12.9% of private payer expenditures are attributable to obesity. Across all payers, results indicate that obesity increases annual medical expenditures by 9.1% or $147 billion per year. Largely due to the rapidly rising rate of obesity, this figure is double the estimate Finkelstein and colleagues generated using similar data from 1998. The publicly funded Medicare and Medicaid programs finance roughly 41% of the total costs attributable to obesity across service categories. Prescription drug expenditures are the largest cost driver, representing 40% of the costs.
As noted in the introduction, there is growing evidence that, in addition to increased medical spending, obese employees have greater rates of absenteeism and presenteeism (Finkelstein, Fiebelkorn, and Wang, 2005; Gates, et al. 2008). In a recent analysis, Finkelstein and colleagues combined multiple data sets to quantify per capita and aggregate estimates of medical expenditures and the value of lost productivity resulting from absenteeism and presenteeism for overweight and Grade I, II, and III obese full time employees (Finkelstein et al. 2010).
Their estimate of presenteeism is based on the validated Work Productivity and Activity Impairment (WPAI) questionnaire. Presenteeism is assessed with the question, “During the past seven days, how much did your health problems affect your productivity while you were working?” Participants indicated their level of work impairment via a rating scale ranging from zero to 10, with zero indicating that “health problems had no effect on my work” and 10 indicating that “health problems completely prevented me from working.” Each response was assumed to represent a percentage reduction in productive work due to health problems—for example, a respondent reporting a value of three is assumed to have a 30% reduction in productive work, whereas a respondent reporting a 10 is assumed to be completely unproductive at work. All results were then annualized and monetized to present estimates of the dollar value of lost productivity.
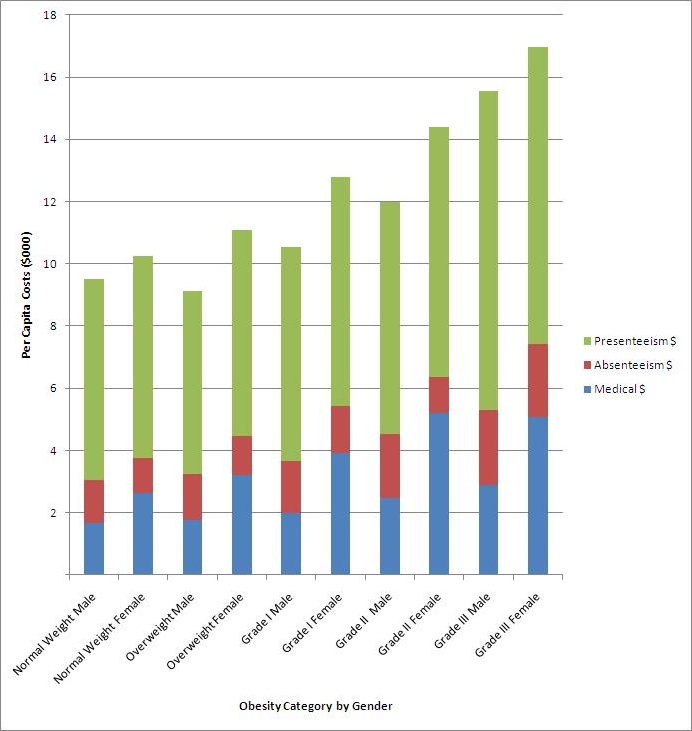
Figure 1 presents the incremental per capita medical expenditures and productivity losses due to each overweight and obesity strata among full time employees separately for men and women. Among men, increases in medical expenditures associated with obesity ranged from $475 more for Grade I to $1,269 more for Grade III obese male employees.
Annual missed workdays ranged from 0.5 more days for overweight men to 5.9 more days for Grade III men, the latter resulting in an annual cost of roughly $1,000. Using the WPAI, presenteeism was shown to be the single largest driver of the costs of obesity for males and to roughly double between each obesity grade. Annualized estimates ranged from 2.3 days for Grade I to 21.9 days for Grade III obese men. The latter estimate equates to roughly one month of lost productivity per year at an average annual cost of $3,792. Across the four categories, per capita obesity-attributable costs ranged from negative $322 for overweight men to $6,087 for Grade III obese men. Results were qualitatively similar for women. Across the four categories, the combined costs of medical expenditures and lost productivity due to absenteeism and presenteeism attributable to obesity ranged from $797 for overweight women to $6,694 for Grade III obese women (Finkelstein et al. 2010).
The authors combined the per capita estimates with obesity prevalence data from full time employees to generate the aggregate costs of obesity. The combined estimated value of medical expenditures, absenteeism, and presenteeism resulting from excess weight among full time employees, which represents roughly 65% of the civilian labor force, were estimated to be $73.1 billion per year; 82% of this expense was roughly equally split between medical expenditures and presenteeism, and 18% resulted from increased absenteeism.
In addition to absenteeism and presenteeism, there is also evidence that obese individuals incur greater indirect costs due to more frequent and more expensive disability and worker’s compensation claims (Trogdon et al. 2008). For example, one unpublished report by UnumProvident Corporation, an insurance provider, found that disability claims attributed to obesity have increased tenfold during the past decade, and that obesity–related disabilities cost employers an average of $8,720 per claim (UnumProvident, 2004). Aggregate costs for these categories are not available.
Although the annual direct and indirect costs of obesity are large, some studies suggest that these estimates may be inflated because they do not account for differences in life expectancy between normal weight and obese individuals (Adams et al. 2006; Flegal et al. 2007). Ironically, premature death from obesity generates a direct medical cost savings, primarily to Medicare which finances the majority of medical costs for those aged 65 and above. Ultimately it is an empirical question whether or not the increase in costs resulting from obesity while alive is offset by reduced life expectancy.
Finkelstein et al. (2008) estimate the lifetime costs of obesity by combining age-, race-, gender- and BMI-specific medical cost and survival data for 20-yr old adults. After discounting future expenditures, lifetime medical costs for Grade I obesity range from $5,340 for black women to $21,550 for white women. For Grades II/III obesity, discounted lifetime medical costs range from $14,580 for black men to $29,460 for white women. One reason why these results may appear smaller than expected is because many of the adverse health consequences of obesity do not occur until individuals are well into adulthood. Discounting these costs from the perspective of an obese 20-year old significantly deflates their value. For example, the cost of obesity from the perspective of a 65-year old Grade III obese white woman is $25,300, which is only slightly lower than the estimate for a 20-year old because from the perspective of a 65-year old, the costs of obesity are immediate.
These estimates focus solely on direct medical costs. Given that the difference in survival rates between obese and normal weight individuals is only a few years on average (Finkelstein et al. 2008) there is little to no ‘savings’ in indirect costs resulting from premature mortality.
The results from these studies reveal that the direct and indirect costs of obesity are large, even from a lifetime perspective. But what are the implications of these findings for the government, which incurs costs through Medicare and Medicaid programs, and for employers who incur costs through lost productivity and increased insurance premiums? Moreover, what can be done to reduce the costs?
From a public policy perspective, classical economists generally believe that the primary role of government is to resolve market failures. Although high costs or prevalence of obesity are not evidence of market failure per se, there may be market failures or distortionary government policies that are responsible for inflating obesity rates and costs beyond what would occur in the absence of these failures. As a result, and given the rapidly rising rates and costs of obesity, it would be appropriate for governments to identify and remediate these failures in efforts to stem the rise in obesity rates and related costs.
Several articles in this Choices theme identify market and government failures in more depth; however one common example is the government subsidy to corn and soybean producers, which ultimately lowers the market price of all animal source foods such as beef, pork, and poultry; products made with high fructose corn syrup, and hydrogenated fats and oils. Some researchers have suggested that the low price of these products is partly responsible for the rise in obesity rates, and that removal of these subsidies could potentially have a positive influence on weight outcomes (Popkin, 2008; Finkelstein and Strombotne, 2010). This topic is discussed further in the article “Farm Policy and Obesity in the United States” found in this issue of Choices.
Beyond market failures, policymakers often use the high costs of obesity to motivate obesity prevention efforts. The most efficient strategy to recover the external costs of obesity would be to experience-rate publicly funded health insurance programs. Experience-rating involves charging obese individuals higher rates based on their higher expected costs. Although this might be infeasible for low-income beneficiaries, a strategy that incorporates experience rating and means testing is feasible and in fact is already being implemented in several public and private health plans (see N.C. state health plan targets smokers and obese, 2009).
In the absence of experience rating, touting the high costs of obesity to justify obesity prevention efforts is only a valid argument if these interventions save more money than they cost. Otherwise the costs of obesity will continue to increase even if the interventions are successful at improving weight and health outcomes. In other words, even cost-effective interventions—those that reduce weight and improve health at a reasonable return—would not be appropriate if the objective is to save money. The requirement for cost savings is an extremely high bar for publicly funded health promotion efforts and may ultimately prove infeasible. This is not to say that efforts should not be made to address obesity, but only that cost savings may not be the appropriate justification.
Finally, in the absence of experience rating, governments are increasingly considering targeted sin taxes as a means to recoup their costs resulting from obesity. While many foods and even nonfood items such as video games or televisions are viable candidates, policymakers are increasingly targeting calorically-sweetened beverages (CSBs) like sodas and sugary sports drinks. Although a number of state and local governments have recently initiated taxes on CSBs, economists disagree over the extent to which these taxes are appropriate (see “Can Taxes on Calorically Sweetened Beverages Reduce Obesity?” in this issue of Choices).
From an employer’s perspective, the high direct and indirect costs of obesity represent a significant cause for concern, yet profit-maximizing strategies for addressing obesity among employees are complicated by several factors. If employers were completely free to set wages, all other things equal, they might adjust wages such that the increased costs of obesity among employees were born entirely by the obese individual. Under this circumstance, the firm bears none of the costs of obesity and should theoretically be indifferent between hiring normal weight or obese employees. Although there is some evidence that obese white women take a wage penalty compared to their normal weight counterparts, there is no evidence of wage adjustments for men or for nonwhite women, suggesting that some of the costs of obesity are borne by the firm (Cawley, 2004; Bhattacharya and Bundorf, 2009). Unions, contracts, minimum wage laws, and the threat of litigation and public backlash all make it difficult for employers to fully adjust wages to offset the costs of obesity. Therefore, employers need to consider alternative strategies for addressing the high rates and costs of obesity among employees.
Because employers are profit-maximizers, an additional challenge for firms is finding obesity interventions that are effective and save money. Many cost-effective obesity interventions that improve health at a reasonable cost are unlikely to receive corporate backing if the interventions do not save money, because most employers will require cost savings, not just cost-effectiveness. Furthermore, due to high job turnover, many firms will be unwilling to substantially invest in obesity prevention and treatment efforts largely on the grounds that some other firm will reap the benefits of these efforts. Investing in employee health made sense 50 years ago when individuals tended to work one or two jobs in their entire career. Today, the average job tenure of private sector employees is less than four years so investments in long-term health are unlikely to show a positive return to the firm. As a result, private sector companies will under-invest in obesity prevention efforts because they receive only a fraction of the benefits from their investment.
The 2010 Affordable Care Act now mandates that large firms offer health insurance to their employees or face a significant financial penalty. Although employer-based coverage and high job turnover reduce incentives for businesses to invest in prevention, firms could benefit from a slimmer, healthier, and perhaps less costly, more productive population if they could be encouraged to make these investments. Ultimately, the encouragement will need to come from the government in the form of direct funding, subsidies, or regulation. This is not only because it is government policy that first encouraged—via tax breaks—and now essentially requires firms to provide health insurance, but also because government has a financial stake in seeing employers implement these efforts given that most employees will eventually become Medicare enrollees. In fact, the federal government may be the single greatest beneficiary of workplace obesity prevention and health promotion efforts. Only time will tell whether or not these efforts prove to be cost-saving, but one thing is certain—without them obesity rates and costs are unlikely to decrease any time in the near future.
Adams, K. F., Schatzkin, A., Harris, T. B., Kipnis, V., Mouw, T., Ballard-Barbash, R., Hollenbeck, A., and Leitzmann, M.F.(2006). Overweight, obesity, and mortality in a large prospective cohort of persons 50 to 71 years old. New England Journal of Medicine, 355(8), 763-778.
Bhattacharya, J., and Bundorf, M. K. (2009). The incidence of the healthcare costs of obesity. Journal of Health Economics, 28(3), 649-658.
Cawley, J. (2004). The impact of obesity on wages. Journal of Human Resources, 32, 451-474.
Field, A.E., Coakley, E.H., Must, A., Spadano, J.L., Laird, N., Dietz, W.H. (2001). Impact of overweight on the risk of developing common chronic diseases during a 10-year period. Archives of Internal Medicine, 161(13), 1581-1586.
Finkelstein, E.A., Fiebelkorn, I.C., and Wang, G. (2005). The costs of obesity among full-time employees. American Journal of Health Promotion, 20(1), 45-51.
Finkelstein, E. A., Trogdon, J.G., Brown, D.S., Allaire, B.T., Dellea, P., and Kamal, B.S. (2008). The lifetime medical cost burden of overweight and obesity: Implications for obesity prevention. Obesity, 16(8), 1843-1848.
Finkelstein, E. A., Trogdon, J. G., Cohen, J. W., and Dietz, W. (2009). Annual medical spending attributable to obesity: Payer-and service-specific estimates. Health Affairs, 28(5), w822-831.
Finkelstein, E.A., and Strombotne, K.L. (2010). The economics of obesity. American Journal of Clinical Nutrition, 91(5), 1520S-1524S.
Finkelstein, E.A., DiBonaventura, M.C., Burgess, S.M., and Hale, B.C. (2010). The costs of obesity in the workplace. Journal of Occupational and Environmental Medicine, 52(9), to be published in 2010.
Flegal, K.M. (1996). Trends in body weight and overweight in the U.S. population. Nutrition Review, 54(4 Pt 2), s97-100.
Flegal, K.M., Graubard, B. I., Williamson, D. F., and Gail, M. H. (2007). Cause-specific excess deaths associated with underweight, overweight, and obesity. Journal of the American Medical Association, 298(17), 2028-2037.
Flegal, K.M., Carroll, M.D., Ogden, C.L., and Curtin, L.R. (2010). Prevalence and trends in obesity among US adults, 1999-2008. Journal of the American Medical Association, 303(3), 235-241.
Gates, D.M., Succop, P., Brehm, B.J., Gillespie, G.L., and Sommers, B.D. (2008). Obesity and presenteeism: The impact of body mass index on workplace productivity. Journal of Occupational and Environmental Medicine, 50(1), 39-45.
Must, A., Spadano, J., Coakley, E.H., Field, A.E., Colditz, G., and Dietz, W.H. (1999). The disease burden associated with overweight and obesity. Journal of the American Medical Association, 282(16), 1523-1529.
Ogden, C.L., Carroll, M.D., McDowell, M.A., and Flegal, K.M. (2007). Obesity among adults in the United States – no statistically significant change since 2003-2004. NCHS Data Brief (1): 1-8.
Pinhas-Hamiel, O., and Zeitler, P. (2007). Acute and chronic complications of type 2 diabetes mellitus in children and adolescents. Lancet, 369(9575), 1823-1831.
Popkin, B.M. (2008). The world is fat – the fads, trends, policies, and products that are fattening the human race. New York, N.Y: Avery-Penguin Group.
Quesenberry, C. P., Jr, Caan, B., and Jacobson, A. (1998). Obesity, health services use, and health care costs among members of a health maintenance organization. Archives of Internal Medicine, 158(5), 466-472.
N.C. state health plan targets smokers and obese (2009, February 9). Available online: http://www.wral.com/news/local/story/4575112/
Sturm, R. (2002). The effects of obesity, smoking, and drinking on medical problems and costs. Health Affairs, 21(2), 245-253.
Thompson, D., Brown, J.B., Nichols, G.A., Elmer, P.J., and Oster, G. (2001). Body mass index and future healthcare costs: A retrospective cohort study. Obesity, 9(3), 210-218.
Trogdon, J. G., Finkelstein, E. A., Hylands, T., Dellea, P. S., and Kamal-Bahl, S. J. (2008). Indirect costs of obesity: a review of the current literature. Obesity Reviews, 9(5), 489-500.
UnumProvident. (2004). Report: Obesity-related disability claims, costs are up. Business and Legal Reports, February 24. Available online: http://hr.blr.com/news.aspx?id=9356.
This article was funded by an internal grant from Duke-NUS Graduate Medical School. No financial disclosures were reported by the authors of this paper.